

Targeted Temperature Management a Clinician's Guide
.png)
The monitor settles. You have a pulse back. Blood pressure is barely holding, the ventilator is running, the team is catching its breath, and someone asks the next high-stakes question.
“Are we doing targeted temperature management?”
That moment is where post-arrest care becomes real. Return of spontaneous circulation is a milestone, not the finish line. The brain has already been through ischemia, and the injury can keep unfolding even after circulation returns. Temperature control is one of the few interventions in this phase that directly aims to protect neurologic recovery.
Introduction A Critical Post-Arrest Intervention
The patient has a pulse again, but the room is still tense. The first few post-ROSC decisions often shape the whole ICU course, and temperature control is one of the ones that still creates the most disagreement at the bedside.
Part of the confusion comes from how many of us were taught this topic. “Cool the post-arrest patient” was easy to remember, but it blurred an important distinction. Current practice is no longer a simple race to 33°C for every comatose survivor. The key question is whether a given patient benefits more from active hypothermia or from meticulous temperature control with strict fever prevention. That debate sharpened after the TTM2 trial, which pushed clinicians to reexamine what improves neurologic outcomes and what may reflect older habits.
That shift matters because TTM is not just a number on an order set. It changes sedation choices, shivering control, electrolyte management, rewarming discipline, and how closely the team watches for fever over the next day or two. In practice, temperature strategy works like a frame around the rest of post-arrest care. If the frame is loose, the whole plan becomes reactive.
A practical review of broader care after cardiac arrest helps place TTM in context. Temperature control sits alongside oxygenation, ventilation, hemodynamics, seizure surveillance, and treatment of the arrest cause. The point is not to treat temperature in isolation. The point is to protect the brain while the rest of the resuscitation continues.
The modern bedside lesson is straightforward. Early hypothermia trials made cooling central to post-arrest care, but newer evidence has narrowed the certainty around aggressive cooling for all patients. What has held up is the need for deliberate temperature control and active fever avoidance in comatose survivors after ROSC. For many clinicians, that has changed TTM from “cool everyone” to “choose a target on purpose, then hold it with discipline.”
TTM succeeds when the team treats temperature as a controlled therapy with a neurologic goal, not as a reflex or a checkbox.
This is also one of those areas where good education changes performance. Clinicians need more than a memorized protocol. They need to understand why targets differ, why shivering can undo the plan, and why rewarming too fast creates problems of its own. That is the kind of structured reasoning many online critical care courses and certification programs, including advanced offerings from ProMed Certifications, are designed to teach in a practical, repeatable way.
What Is Targeted Temperature Management
Targeted temperature management is the deliberate control of a patient's core temperature after cardiac arrest to reduce secondary brain injury. It isn't accidental hypothermia, and it isn't a mere command to 'make the patient cold.' It's a controlled physiologic intervention with a neurologic goal.
Think of it as a metabolic brake. After the heart restarts, the brain doesn't instantly return to normal. Cells that were starved of oxygen begin a second wave of injury when blood flow returns. That reperfusion phase can trigger inflammation, oxidative stress, and swelling. Temperature control slows that injury environment down.
Why temperature affects the brain
The physiologic logic matters because it helps you remember why each step in the protocol is so strict. The Neurocritical Care guideline describes evidence from preclinical models showing that the thermal range used in TTM can reduce reactive oxygen species production, reduce mitochondrial membrane permeability, and reduce inflammatory cytokine release, while helping preserve the blood-brain barrier in post-arrest care according to the Neurocritical Care TTM guideline.
That same guidance also notes a vasoconstrictive response with lower core temperature that can help decrease intracranial pressure by limiting vasogenic edema. You don't need to memorize every mechanism to use TTM well, but you do need to understand the central idea. Controlled temperature can create a more favorable recovery environment for an injured brain.
What TTM is not
A few misunderstandings come up often:
- It's not random cooling. If the patient's temperature drifts down or up without control, that's not TTM.
- It's not only about hitting one number. The number matters, but consistency matters too.
- It's not separate from the rest of ICU care. Sedation, analgesia, ventilation, hemodynamics, and lab monitoring all affect how well TTM works.
For many learners, this is also one of those topics that benefits from replay and review. That's one reason online programs are so useful for certification prep. If you're refreshing post-arrest management in ACLS Certification, an online format lets you revisit algorithms, pacing, and protocol details when you have time to focus. ProMed Certifications offers a quick and convenient way to get ACLS-certified, and the course can be taken anywhere within a busy schedule.
Practical rule: If you can't explain the “why” of cooling, rewarming, and fever prevention, the bedside steps will feel harder than they are.
Who Needs TTM Patient Selection and Indications
A common post-arrest scene goes like this. The patient has a pulse, the blood pressure is barely acceptable, the team is catching its breath, and then someone asks, “Are we cooling?” That question matters, but the better first question is simpler. Can this patient follow commands after return of spontaneous circulation?
That bedside moment is where patient selection starts. TTM is aimed at the patient whose heart has restarted but whose brain has not clearly re-engaged. If the patient is awake, tracking, and following commands, induced hypothermia is usually not the issue. If the patient remains comatose, temperature control becomes part of brain-focused post-arrest care.
The patients who belong in the discussion
The clearest adult candidates are patients who remain unresponsive after ROSC, whether the arrest happened out of hospital or in hospital. The location matters less than the neurologic state in front of you. A patient with spontaneous circulation and no meaningful response to verbal commands should trigger a temperature plan.
That point is easy to miss because older teaching often framed TTM as a cooling decision. Current practice is more precise. The primary decision is whether this comatose post-arrest patient needs active temperature control, and whether that means hypothermia or strict fever prevention.
The modern debate matters here. Earlier eras pushed many teams toward 33°C almost by reflex. The TTM2 trial shifted that reflex. In adults who were comatose after out-of-hospital cardiac arrest, cooling to 33°C did not show a survival or functional advantage over active fever prevention. At the bedside, that means your candidate pool still includes comatose post-ROSC patients, but your goal is no longer “cool everyone hard.” Your goal is controlled temperature management, with particular attention to avoiding fever.
Practical bedside indications
Use a screening approach that is fast enough for the first few minutes and focused enough to avoid confusion:
- Has the patient achieved ROSC?
- Are they still comatose or unable to follow commands?
- Can they tolerate active temperature control, or do competing problems change the plan?
This works like a triage lens. The first question confirms you are in post-arrest care. The second identifies the patients most likely to need neuroprotective temperature management. The third keeps you from applying protocol language to a patient whose immediate danger is something else.
When to slow down and individualize
Some patients fit the indication but still make you pause. Active bleeding, marked hemodynamic instability, or another urgent problem that needs immediate correction can change how aggressively you pursue hypothermia. In those cases, strict fever prevention may be the safer and more realistic target.
Patients who arrive already hypothermic also need a different frame of mind. You are not deciding whether to start cooling from scratch. You are deciding how to manage the temperature they already have without causing harm through uncontrolled rewarming. That is one of the places where protocol discipline matters. Sudden swings in temperature can undo the benefit of careful post-arrest care.
Another source of confusion is the patient with a grim exam in the first hour. Early coma alone should not be mistaken for futility. Sedatives, residual paralysis, shock, and the arrest itself can all cloud the neurologic picture. For that reason, a comatose patient after ROSC usually deserves active temperature planning unless there is a clear reason not to provide it.
What this means in the TTM2 era
The practical lesson from newer evidence is not that temperature stopped mattering. It is that indiscriminate deep cooling is harder to justify than it once was. Many adult post-arrest patients still meet indications for TTM because they are comatose after ROSC. What has changed is the bedside emphasis. Strict prevention of fever is now central, and selected patients may still be managed with lower targets based on local protocol, clinician judgment, and the full clinical picture.
So the selection question is best phrased this way: Is this a comatose post-arrest patient who needs active temperature control to protect the brain? If the answer is yes, you are in the right lane. The next step is choosing the target strategy carefully, rather than assuming every patient needs the same degree of cooling.
Defining the Target Temperature and Timing
A common ICU moment goes like this. The postarrest patient arrives intubated, sedated, and unresponsive. One clinician says, “We cool to 33.” Another says, “TTM2 changed that.” If the team does not share the same frame, the patient can spend the next several hours drifting in temperature while everyone debates the target.
That uncertainty is the core problem.
The practical question is no longer whether temperature control matters. It does. The harder question is what you are trying to accomplish at the bedside. Are you trying to gain benefit from active hypothermia, or are you making sure the patient never develops fever after a global ischemic brain injury? Modern TTM practice starts by separating those two ideas clearly.
How the target range evolved
For years, many ICUs treated 33°C as the standard destination. That approach came from earlier trials suggesting benefit from cooling after cardiac arrest, and it shaped training for a generation of clinicians. The protocol felt straightforward. Pick 33, get there promptly, hold it, then rewarm carefully.
Later studies and guideline updates broadened that view. Current guidance generally accepts a controlled core temperature somewhere in the 32°C to 36°C range, maintained for at least 24 hours, with continued attention to fever after the maintenance phase. In practical terms, the field shifted from a single temperature to a temperature-control strategy.
That change can feel subtle on paper and major at the bedside. A fixed target of 33°C asks the team to induce hypothermia. A target near 36°C asks the team to prevent the patient from passively warming into fever. Both require planning, monitoring, and shiver control, but they are not the same physiologic intervention.
What the newer evidence changed
The TTM2 trial sharpened this debate. Its message was not that temperature stopped mattering. Its message was that, in many comatose adult postarrest patients, routine cooling to 33°C did not show a clear outcome advantage over a strategy centered on active fever prevention.
That is why recent recommendations place so much emphasis on avoiding fever. ILCOR now frames the issue around active prevention of fever, rather than assuming every patient should undergo aggressive hypothermia. For bedside practice, that is a meaningful shift. It lowers the threshold for saying, “This patient needs disciplined temperature control,” while raising the threshold for saying, “This patient automatically needs deep cooling.”
A simple way to teach this is to compare TTM to ventilator management. You would not say, “The patient is intubated, so any mode is fine.” You choose settings based on the physiology you are trying to control. Temperature management works the same way. The target should reflect a deliberate strategy, not habit.
Choosing a target in real practice
A reasonable bedside approach today looks like this:
- Set an active temperature goal early
- Treat fever prevention as a core part of neuroprotection
- Use lower targets selectively, based on patient factors, local protocol, and clinician judgment
- Continue temperature control after the initial maintenance period so rewarming does not end in rebound hyperthermia
This is why thoughtful clinicians can choose different targets and still practice good medicine. One team may favor strict normothermia with aggressive fever prevention. Another may choose a lower target for a specific patient because of local experience, perceived neurologic risk, or protocol design. The quality marker is not uniformity. It is whether the team chose a target on purpose and can carry it out reliably.
Why timing still matters
Timing matters because brain injury after ROSC is not a single event. It is an evolving process of reperfusion injury, inflammation, metabolic stress, and secondary insults. Temperature swings feed that process. Delay gives fever a chance to appear before your protocol does.
The practical lesson is simple. Decide early, measure core temperature accurately, and start controlled management before the patient starts bouncing between passive cooling, warming blankets, shivering, and reactive medication pushes. A sloppy start makes the rest of TTM harder.
Rewarming deserves the same discipline. If cooling is the braking phase, rewarming is taking your foot off the brake on an icy road. Done slowly and deliberately, it is stable. Done casually, it can bring vasodilation, electrolyte shifts, hemodynamic instability, and rebound fever. Many protocol failures happen here, not during the initial cooling period.
The modern debate, then, is not “33°C versus nothing.” It is aggressive hypothermia versus strict fever prevention with active control. TTM2 pushed practice toward the second approach for many adults, but it did not give permission for temperature drift. The patient still needs a target, a clock, and a team that understands why both matter.
The TTM Protocol A Step by Step Guide
You get ROSC at 2:10 a.m. The room is noisy, the blood pressure is drifting, and everyone is doing the right task in isolation. What the patient needs now is coordinated temperature control. A good TTM protocol turns a tense post-arrest hour into a sequence the whole team can follow.
The bedside goal is straightforward. Pick the temperature strategy your unit intends to deliver, reach it in a controlled way, hold it with as little drift as possible, and prevent fever afterward. That approach fits both sides of the modern debate. Units that still choose lower-temperature hypothermia need disciplined execution, and units that follow the TTM2-era shift toward active normothermia still need the same discipline because fever prevention fails when no one owns the process.
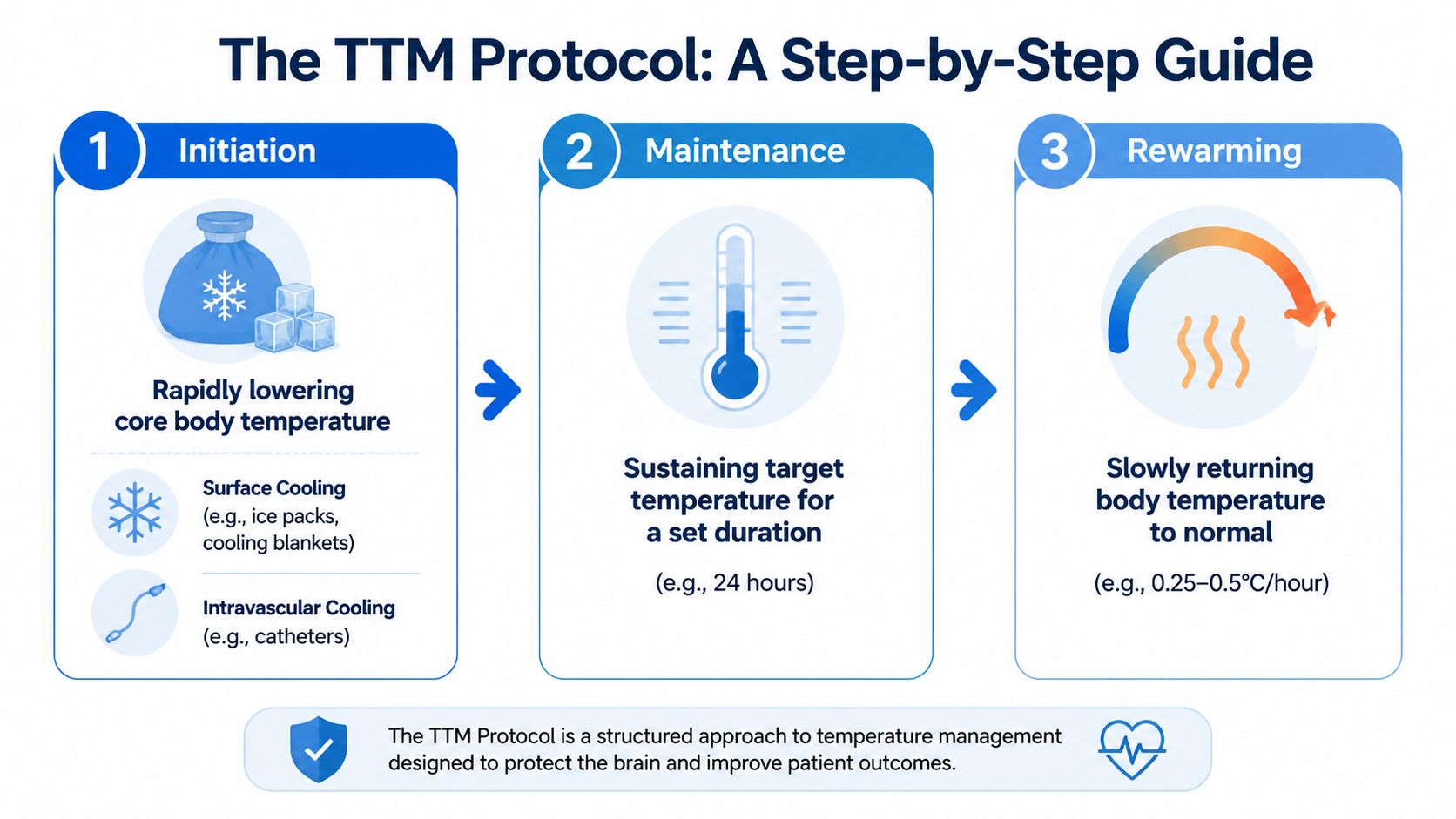
Initiation
Initiation begins with a clear order set and a clear voice at the bedside. Someone needs to say the target out loud, confirm how it will be measured, and assign the first steps. If that sounds basic, it is. It also prevents the common early mistake of having three people "cooling" the patient in three different ways without a shared endpoint.
Cooling methods differ by resources and experience. Ice packs and simple external measures can start temperature reduction, but device-based systems with servo-control usually make bedside care more predictable because they adjust continuously instead of relying on repeated manual corrections. The practical point is precision. The less the temperature swings early, the easier the rest of the protocol becomes.
Maintenance
Maintenance is where a protocol proves whether it is real or only written in the chart. Reaching the target gets attention. Holding it steadily protects the patient.
The easiest way to teach this phase is to compare it to ventilator management. You would not accept a patient whose oxygen saturation swung widely all day because the vent was "mostly on target." Temperature control deserves the same mindset. Small drifts trigger shivering, extra sedation, more nursing interventions, and more metabolic stress.
During maintenance, the team should keep returning to four questions:
- Is the core temperature measurement reliable? Bladder, esophageal, or other true core monitoring is better than surface guesswork.
- Is shivering being treated early? Waiting for obvious shaking is late recognition.
- Are analgesia and sedation matched to the temperature plan? An uncomfortable patient will resist cooling.
- Does every discipline know the same target and timeline? Mixed messages create temperature variability.
This is also the point where the hypothermia-versus-fever-prevention debate becomes practical rather than theoretical. If your protocol target is 33°C, maintenance means tightly controlled cooling and close shiver management. If your protocol target is active normothermia, maintenance still means active control, not passive observation. TTM2 shifted many ICUs away from routine deep hypothermia, but it did not make temperature management optional.
Rewarming
Rewarming needs the same respect as initiation. It works like easing off the brakes on a downhill road. If you do it too quickly, the patient can drift into hypotension, electrolyte instability, and rebound fever before the team catches up.
A controlled rewarming plan should be written, timed, and visible to the bedside nurse. Passive warming invites overshoot. Controlled warming keeps the team ahead of the physiology instead of reacting after the fact.
One practical teaching point matters here. TTM is not finished when the patient reaches normothermia. The post-rewarming period is where sloppy protocols declare victory too early and then lose temperature control a few hours later.
Here is the bedside sequence I teach residents and new ICU nurses:
- State the target clearly and document it
- Use the most precise temperature-control method available
- Confirm true core temperature monitoring
- Prevent and treat shivering before it escalates
- Maintain the target with minimal drift
- Rewarm slowly and deliberately
- Continue active fever surveillance after rewarming
That sequence keeps the protocol simple under pressure and aligns with current bedside practice. Whether your unit chooses lower-temperature cooling for selected patients or prioritizes strict fever prevention after TTM2, the skill is the same. Run the process on purpose, not by drift.
Managing Complications and Patient Monitoring
Targeted temperature management can protect the brain, but it also changes nearly every other system you're managing. The safest teams are the ones that expect complications before they show up.

What usually causes trouble
Shivering is the most visible problem. It directly opposes cooling and increases metabolic demand. If a patient is visibly shaking, your temperature protocol is no longer just a temperature protocol. It has become a comfort, sedation, and metabolic management problem.
Electrolyte shifts are less obvious but just as important. Potassium, magnesium, and phosphate can move during cooling and again during rewarming. That means labs that looked manageable earlier can become dangerous later if the team isn't watching trends.
You also need to keep an eye on:
- Hemodynamics
- Cardiac rhythm
- Coagulation concerns
- Signs of infection
- Glucose control
- Sedation depth and neurologic exam limitations
Monitoring that matters most
A good TTM setup usually includes a few essential components:
- Reliable core temperature monitoring
- Continuous cardiac and hemodynamic monitoring
- Frequent laboratory review
- Regular assessment for shivering and skin issues
- A shared plan for sedation, analgesia, and ventilator synchrony
The broader post-cardiac-arrest care overview is useful here because it reminds teams that temperature management sits inside a larger ICU framework. If blood pressure, oxygenation, or ventilation are off, TTM alone won't rescue the neurologic picture.
Practical bedside habits
The units that do this well tend to use habits rather than heroics:
- Say the target out loud. Everyone should know whether the goal is lower hypothermia or strict normothermia.
- Document the phase. Initiation, maintenance, and rewarming each have different priorities.
- Treat shivering early. Waiting until it's obvious makes control harder.
- Watch the patient after rewarming. Fever prevention still matters once the cooling phase is done.
One more point often gets missed. Sedated, cooled patients can look deceptively stable. Don't let that appearance lower your vigilance. TTM patients need more disciplined monitoring, not less.
Key Trials and Guideline Recommendations
A patient arrives in the ICU after ROSC. The team is organized, the airway is secured, blood pressure is being supported, and then the familiar question comes up. Do we cool to 33°C, or is careful fever prevention enough?
The trials that shaped current practice
That question sits at the center of the modern TTM debate. Earlier studies helped establish hypothermia as a standard part of post-arrest care, so many clinicians were taught that lower temperatures were more protective. Later trials tested that assumption more directly. The core issue was whether benefit came from aggressive hypothermia itself or from preventing fever and avoiding temperature swings in an injured brain.
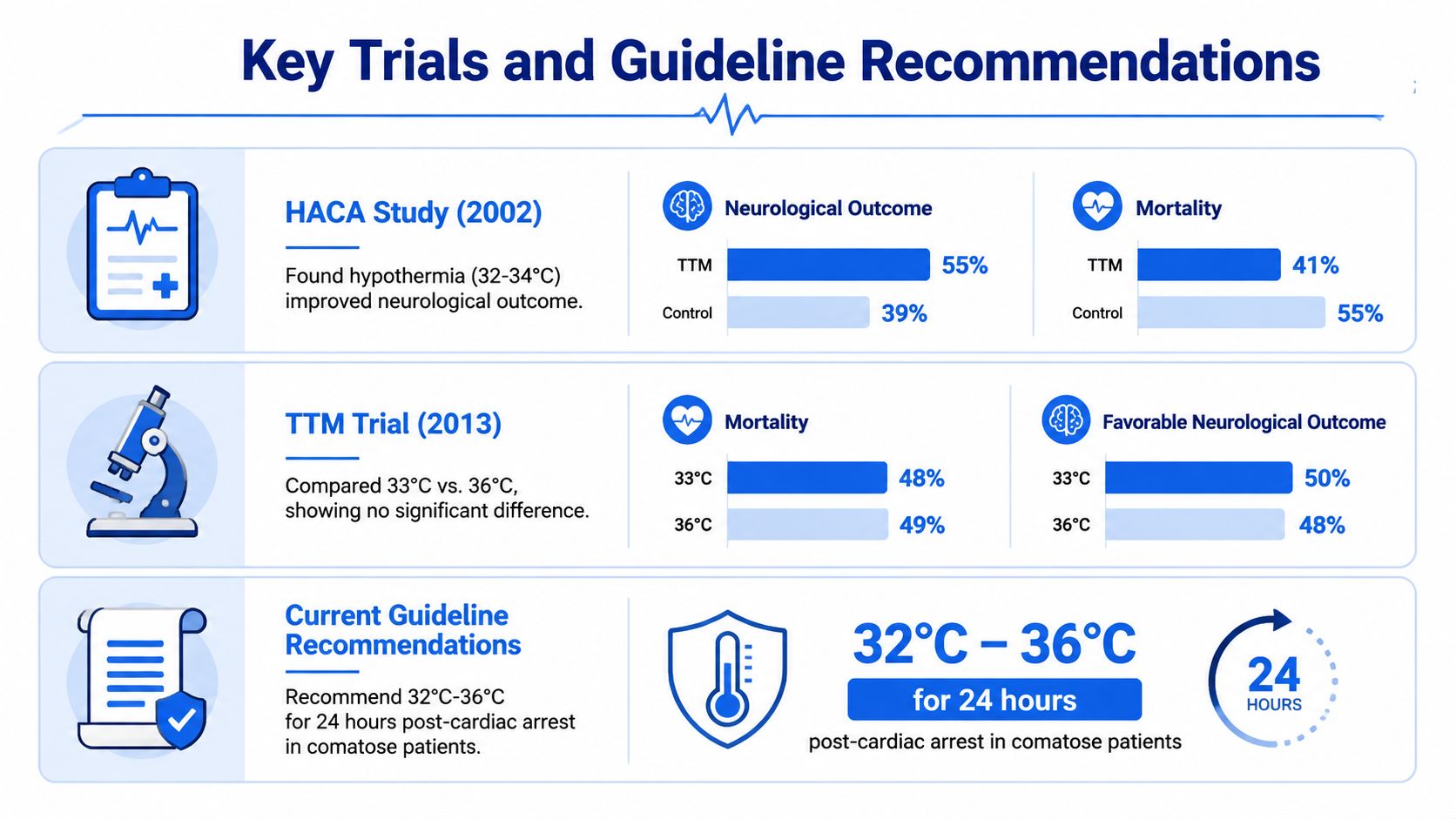
The TTM trial compared 33°C with 36°C and found no significant mortality difference, according to the American College of Cardiology review of major TTM evidence. For many bedside clinicians, that was the first strong signal that precise control might matter more than pushing every patient to deeper cooling.
The TTM2 trial sharpened the point. Patients were assigned to hypothermia at 33°C or targeted normothermia with active treatment of fever. Outcomes were similar between groups. The same review notes no significant difference in survival or severe disability. That result did not make temperature management less important. It changed what many clinicians now believe the treatment is accomplishing.
A practical way to frame it is this. The post-arrest brain often behaves like tissue that has lost its ability to regulate heat well. Fever can add metabolic stress at exactly the wrong time. TTM, in modern practice, works less like a universal mandate to cool extensively and more like a disciplined strategy to keep temperature from becoming another injury.
What the guidelines now emphasize
Current guidelines reflect that shift in thinking. They still support active temperature management in comatose patients after cardiac arrest, but they no longer treat routine deep hypothermia as the default answer for everyone.
At the bedside, that usually means focusing on a few core principles:
- Choose a deliberate temperature target rather than letting temperature drift
- Maintain active temperature control for at least 24 hours when TTM is used
- Prevent fever after the initial temperature-control period
- Reserve lower targets for cases where the team believes the potential benefit outweighs the added complexity and risk
That last point is where people often get tripped up. The debate is not whether temperature matters. Temperature clearly matters. The debate is whether pushing to 33°C improves outcomes enough, across broad patient groups, to justify more sedation, more shivering control, more electrolyte shifts, and a more complicated ICU course than strict normothermia requires.
For a bedside framework that connects this evidence to workflow, the ACLS post-cardiac-arrest care algorithm for post-arrest management is a useful reference. It places temperature control in the full resuscitation picture, alongside ventilation, hemodynamics, coronary evaluation when indicated, and neurologic support.
Education matters here because old teaching can linger long after practice changes. Clinicians who trained in the era of routine hypothermia may still picture TTM as synonymous with cooling to 32°C to 34°C. Current guidance is more nuanced. It asks teams to use temperature control with intention, prevent fever reliably, and choose deeper hypothermia selectively rather than automatically.
Conclusion Putting TTM Into Practice With Confidence
Targeted temperature management gets easier once you stop treating it like a mysterious ICU ritual. It's controlled temperature strategy after ROSC for a brain that has been injured and is still vulnerable.
The key bedside ideas are straightforward. Choose the right patient. Set a clear target. Maintain it carefully. Control shivering. Rewarm deliberately. Prevent fever afterward. Most errors happen when the team treats one of those steps as optional.
The biggest change in recent years is not that TTM disappeared. It didn't. The change is that clinicians now think more carefully about whether the benefit comes from routine deep hypothermia or from disciplined fever prevention and precise temperature control. That's a more nuanced view, and it matches what many bedside teams are seeing in practice.
This is exactly the kind of topic that rewards ongoing education. Critical care protocols change. Trial data evolves. Algorithms get updated. You don't need to sit in a hotel conference room to keep up. High-quality online certification and CE can teach advanced post-arrest thinking just as effectively as in-person formats, with far more flexibility for working nurses, physicians, and other clinicians. The old idea that only AHA or Red Cross in-person courses count is outdated. Healthcare education is broader than that now, and many institutions recognize accredited online options.
If you want to feel more confident when the post-ROSC questions start flying, keep studying the evidence and keep practicing the workflow. TTM rewards clinicians who are calm, current, and systematic.
If you're ready to refresh advanced resuscitation knowledge in a flexible format, ProMed Certifications offers online certification and continuing education options for healthcare professionals who need current, accessible training without giving up clinical time.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)
.png)