

A Modern Guide to Care After Cardiac Arrest

Once a patient gets a pulse back after cardiac arrest, the real work begins. The care that follows is a rapid, coordinated effort focused on one primary goal: preserving brain function and stabilizing the patient. This initial window, known as the post-cardiac arrest phase, is all about optimizing ventilation, managing blood pressure, and hunting down the root cause of the arrest. This guide will help you navigate the critical steps involved in giving every patient the best possible chance at a meaningful recovery.
The Critical First Hour After ROSC
When a patient achieves Return of Spontaneous Circulation (ROSC), an invisible clock starts ticking. This first hour isn't just about keeping the pulse you worked so hard to get back; it's about laying the groundwork for a meaningful neurological recovery.
Every action we take during this period directly impacts the brain's ability to heal after being starved of oxygen. Think of it as the controlled calm after the storm, where the organized chaos of resuscitation gives way to meticulous, goal-directed therapy.
The progress in this field has been astounding. Over the last five decades, survival rates have seen massive improvements thanks to better emergency response and medical treatments. For instance, survival rates for in-hospital heart attacks have skyrocketed from around 60% in 1970 for older patients to over 90% more recently, especially for younger individuals. This incredible progress, detailed in trends from med.stanford.edu, shows that while we're getting better at the initial save, long-term management is where the next big challenge lies.

Immediate Priorities Following ROSC
Right after ROSC, the mission is twofold: prevent secondary brain injury and stabilize the patient's hemodynamics. This requires a multi-front attack that goes far beyond basic life support and into advanced critical care.
- Optimize Ventilation and Oxygenation: If it's not already done, the first move is securing the airway, usually with an endotracheal tube. The sweet spot for oxygen saturation is between 92-98%, and we aim for normocapnia (a PaCO2 of 35-45 mmHg). It's a delicate balance—both hypoxia and hyperoxia are toxic to the recovering brain, so we have to be vigilant with the FiO2.
- Manage Hemodynamics: It's incredibly common for these patients to be hypotensive, and that's a major threat. The immediate goal is a systolic blood pressure >90 mmHg and a mean arterial pressure (MAP) >65 mmHg. This almost always requires a fluid bolus and, more often than not, a vasoactive drip like norepinephrine or epinephrine to support their pressure.
- Obtain a 12-Lead ECG: This is non-negotiable and needs to happen ASAP. The post-ROSC ECG is our best tool for spotting an ST-segment elevation myocardial infarction (STEMI), a very common culprit behind cardiac arrest. A "hot" ECG means a direct trip to the cath lab for emergent intervention.
- Identify and Treat Reversible Causes: Remember the "H's and T's"? They're still in play. We need to quickly rule out things like Hypovolemia, Hypoxia, Hydrogen ion (acidosis), Hypo/hyperkalemia, and Hypothermia. And don't forget the T's: Tension pneumothorax, Tamponade, Toxins, and Thrombosis. A quick point-of-care ultrasound (POCUS) can be invaluable here for spotting issues like tamponade or a massive PE.
A structured approach is everything. Following a clear, step-by-step framework ensures that all these critical tasks are handled quickly and in the right order, leaving nothing to chance.
To help keep these initial, high-stakes actions organized, here’s a quick-reference table summarizing the priorities.
Immediate Post-ROSC Stabilization Priorities
This table breaks down the key interventions and goals your team should focus on within the first hour of achieving ROSC.
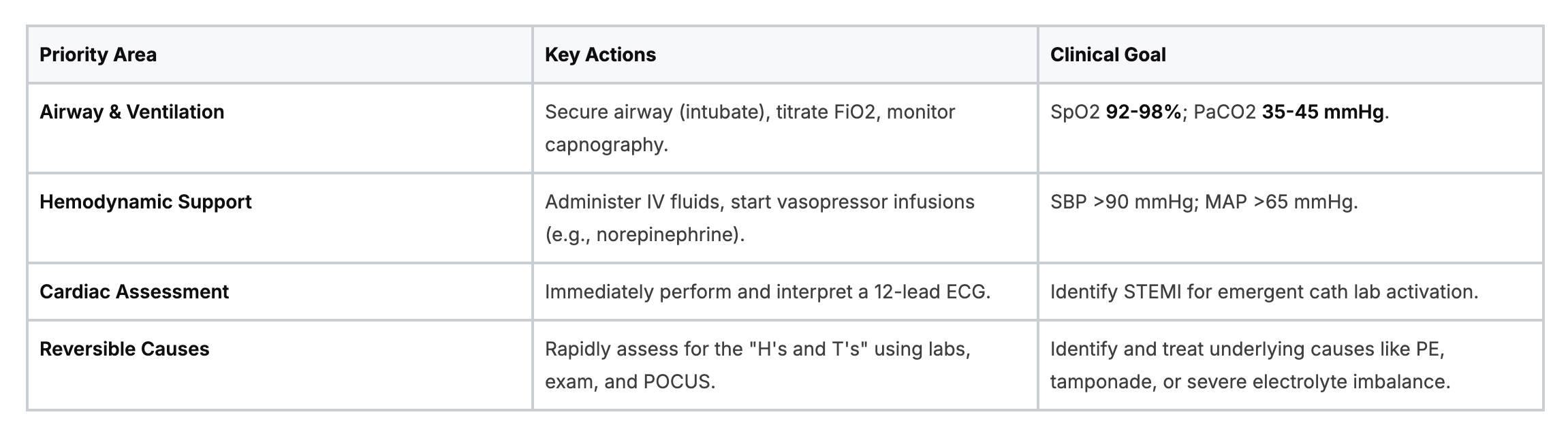
Think of this table as your cognitive offload tool in a high-stress situation. It ensures the foundational elements of post-arrest care are covered before moving on.
The Shift to Advanced Care
Once these initial fires are put out, the focus broadens. We start thinking about more advanced therapies like Targeted Temperature Management (TTM). For comatose patients, initiating the cooling process early can be neuroprotective. This doesn't mean the full protocol is done in an hour, but it does mean getting the cooling devices ready and starting the process to bring the patient's core temperature down to between 32-36°C.
Securing better vascular access, like placing a central line, also becomes a priority. It's crucial for administering multiple medications and getting more accurate hemodynamic monitoring. This first hour is intense and requires constant re-evaluation, but it truly sets the tone for the patient’s entire hospital stay and their ultimate shot at a good recovery.
You can dive deeper into the specific steps and sequences in our guide on the ACLS post-cardiac arrest care algorithm.
Optimizing Hemodynamic and Cardiovascular Support
Getting a pulse back is just the start. Now the real work begins. We need to meticulously manage the patient's hemodynamics—optimizing blood pressure, cardiac output, and tissue perfusion to shield the vital organs, especially the brain.
After a cardiac arrest, the cardiovascular system is incredibly fragile. We call this post-cardiac arrest syndrome, a messy state of myocardial stunning, systemic inflammation, and persistent shock. Your immediate focus has to be on stabilization.
The magic number here is a mean arterial pressure (MAP) of at least 65 mmHg. This isn't just a random target; it’s the minimum pressure required to keep blood flowing adequately to the brain and other crucial organs. If the MAP dips below this, you risk a secondary ischemic injury, which can completely undo all the hard work you just put into the resuscitation.
Choosing the Right Vasoactive Medications
Hypotension is public enemy number one in post-arrest care, and you’ll almost always need vasoactive drugs to combat it. Picking the right one is like a mechanic choosing the right tool—it has to fit the specific job.
- Norepinephrine (Levophed): This is your go-to, first-line vasopressor for most post-arrest patients. Its powerful alpha-adrenergic effects crank up systemic vascular resistance, which brings the blood pressure up effectively. It also gives a little beta-adrenergic support to the heart without sending the heart rate through the roof and overtaxing the myocardium.
- Epinephrine: This drug is a hero during the arrest, but its role after ROSC is a bit more complicated. Its strong beta-agonist effects can cause wicked tachycardia and skyrocket myocardial oxygen demand—not ideal for a heart that's already stunned and battered. That said, it has its place. In cases of severe cardiogenic shock or profound bradycardia where you need both contractility (inotropic) and heart rate (chronotropic) support, it can be a lifesaver. You can dive deeper into its uses in our article on the role of epinephrine in cardiac care.
- Dobutamine: What if the blood pressure is okay, but the heart just isn't pumping well? If you see signs of poor cardiac output—like a low ejection fraction on a bedside echo or cold peripheries despite a decent MAP—it's time to think about an inotrope. Dobutamine is a great choice here. It primarily boosts the heart's contractility with less of an impact on blood pressure.
The bottom line is to tailor your approach to the type of shock you're seeing. Is it distributive shock from a massive inflammatory response? Or is it cardiogenic shock from a stunned myocardium? Your choice of pressor needs to match that clinical picture.
Advanced Monitoring for Precise Adjustments
Managing hemodynamics isn't a "set it and forget it" kind of deal. It demands constant vigilance and frequent tweaks based on what the patient is telling you through the monitors.
An arterial line is non-negotiable for these patients. It gives you a continuous, beat-to-beat blood pressure reading, which is infinitely more accurate and responsive than a cuff pressure that cycles every few minutes. This allows you to fine-tune your vasopressor drips with precision, hitting that target MAP without overshooting or letting it dip.
Regular lab draws are also key. Getting a comprehensive metabolic panel gives you a snapshot of what’s happening internally, guiding your next moves. I always pay close attention to serial lactate levels. A rising lactate is a major red flag for poor tissue perfusion and cellular hypoxia, even if the MAP looks pretty. Conversely, seeing that lactate start to "clear" is one of the most reassuring signs that your resuscitation strategy is working.
Takeaway: Your hands-on clinical assessment is still king. Cold extremities, a sluggish capillary refill, and dropping urine output are all classic signs of poor perfusion that a monitor can't always capture. Always, always treat the patient, not just the numbers on the screen.
The Delicate Balance of Fluid Management
Finally, let's talk about fluids. This is a real balancing act. While you often need to give some fluid boluses upfront to correct hypovolemia, going overboard can be just as dangerous. Post-arrest patients have leaky capillaries from the systemic inflammatory response, putting them at high risk for pulmonary edema and ARDS.
The goal is euvolemia—a state of perfect fluid balance. Before you hang another bag, use dynamic assessments like a passive leg raise or an ultrasound of the inferior vena cava (IVC) to see if the patient will even respond to more fluid.
Once things have settled down, it’s usually better to lean on your vasopressors to maintain blood pressure rather than continuing to pour in fluids. This strategy supports organ perfusion while dramatically lowering the risk of fluid overload, a nasty complication that can really worsen outcomes.
Implementing Targeted Temperature Management
When it comes to neuroprotective care after a cardiac arrest, Targeted Temperature Management (TTM) is one of our most powerful tools. For any comatose patient, proactively cooling the body is a proven strategy to shield the brain from secondary injury. It's a game-changing intervention, but it's one that demands absolute precision from beginning to end.
The idea behind it is pretty straightforward: cooling the brain slows down its metabolic rate. It’s a bit like putting an overheating computer into a low-power mode to prevent damage. By dropping the body's core temperature, we slash the brain's hunger for oxygen and energy, buying it critical time to recover from that initial ischemic hit. This also helps pump the brakes on the damaging inflammatory cascade that kicks in after reperfusion.
To pull this off effectively, your team needs to be sharp, confident, and well-versed in the latest evidence. This isn't just about knowing the steps; it's about understanding the 'why' behind them.
The Three Phases of TTM
Executing TTM isn't a single action but a structured process broken down into distinct stages. Each phase comes with its own goals, challenges, and need for constant vigilance.
- Induction: This is the race to cool. The goal is to get the patient’s core temperature down to the target range of 32-36°C as fast as you safely can. Your options range from low-tech external methods like ice packs and cooling blankets to more advanced setups like surface cooling pads or internal catheter-based systems.
- Maintenance: Once you hit your target temperature, the real work begins. Now you have to hold it steady, typically for at least 24 hours. The biggest fight here is preventing temperature swings and managing the body’s reflexive attempt to warm itself up—shivering.
- Rewarming: This might be the most delicate part of the whole process. You have to rewarm the patient slowly and with extreme control, usually no faster than 0.25°C per hour. Going too fast can unleash a storm of complications, including dangerous electrolyte shifts, cerebral edema, and severe hemodynamic instability.
The infographic below really drives home the point that this is a continuous cycle of monitoring, intervening, and reassessing.
Post-arrest care is never a "set it and forget it" protocol. It's a dynamic process that requires you to constantly adapt to how your patient is responding.
Managing Shivering and Sedation
Shivering is public enemy number one during TTM. It's the body's natural defense against cold, but in this context, it's completely counterproductive. Shivering jacks up the metabolic rate and oxygen demand, wiping out the very benefits you're trying to achieve with cooling. Aggressively managing shivering isn't just a good idea—it's non-negotiable.
The best way to tackle it is with a multi-pronged attack:
- Surface Counter-warming: It sounds strange, but applying warming blankets to the patient's hands and feet can trick the body. The peripheral sensors feel warm, which helps dampen the central drive to shiver.
- Pharmacological Management: Scheduled acetaminophen is a good start. Adding medications like buspirone can also help suppress the shiver reflex.
- Sedation: You'll almost always need deep sedation. Propofol and dexmedetomidine are go-to choices because they not only sedate the patient but also have inherent anti-shivering properties.
Key Takeaway: The goal is to stop the shiver without sedating the patient so heavily that you can't perform a meaningful neurological assessment later. It's a fine line to walk and requires constant clinical judgment.
If you want to get deeper into the physiology of cooling, our guide on the complexities of hypothermia offers some great additional insights.
Training and Certification in Modern Healthcare
Successfully managing a complex protocol like TTM depends on top-notch, continuous education. In the past, this meant blocking off days to attend in-person classes, which is a huge challenge for any busy clinician. Thankfully, the way we learn has changed for the better.
Numerous peer-reviewed studies have confirmed that online education is just as effective as traditional classroom training—and sometimes even better for knowledge retention. Because the outcomes for patient care are equivalent, hospitals and healthcare systems are increasingly accepting accredited online certifications.
The old mindset that only certifications from a few legacy organizations like the AHA or American Red Cross are valid is quickly becoming a thing of the past. The reality is that high-quality, accredited online providers deliver education that is perfectly aligned with the latest clinical guidelines. ProMed is leading this change, offering modern courses that give you both convenience and credibility. Our online platform makes it possible to stay current on critical skills like ACLS without having to sideline yourself from your demanding schedule.
Navigating Neurological Monitoring and Prognostication
Trying to predict a patient's neurological future after cardiac arrest is easily one of the toughest, most emotionally charged parts of the job. You've fought tooth and nail to bring them back, and now the biggest question looms: what will their recovery actually look like?
This isn't about finding one magic test. It’s about building a case, piece by piece, over time. Think of yourself as a detective, gathering a mosaic of clinical evidence. Every bit of data—from a simple physical exam to advanced diagnostics—adds another layer to the story. And remember, no single finding should ever be used in isolation to call it.
The Cornerstone of Serial Clinical Exams
Your most powerful tool, especially in those first crucial 72 hours, is your own hands-on clinical assessment, repeated over and over. Something as basic as checking pupillary light reflexes, corneal reflexes, and motor responses to pain gives you invaluable, real-time feedback on brainstem and cortical function.
If a patient still has no pupillary or corneal reflexes at 72 hours or later, it’s a strong predictor of a poor outcome. The same goes for a motor response that never gets better than extensor or flexor posturing. On the flip side, seeing those reflexes return early or watching a patient start to localize to pain offers a real glimmer of hope.
Key Insight: Don't get fooled by confounders. Sedation and hypothermia will suppress these neurological responses. It's absolutely critical to perform these exams only when the patient is normothermic and has had time off sedatives, giving you the "cleanest" possible assessment.
The Role of Continuous EEG Monitoring
Beyond what you can see at the bedside, continuous electroencephalography (EEG) is a non-negotiable part of modern post-arrest care. It’s a direct window into the brain's electrical activity, and its main job is to hunt for a hidden enemy: non-convulsive seizures. These silent seizures can silently worsen the initial brain injury and must be caught and treated aggressively.
EEG also reveals background patterns that tell us a lot. Malignant patterns like burst-suppression or a flat, suppressed background that just won't budge for over 24 hours are strongly linked to poor outcomes. But if you see that background activity return to a continuous, reactive state, that’s an encouraging sign that the brain may be on the road to recovery.
Integrating Advanced Prognostic Tools
As you push past that initial 72-hour window, other tools can add critical pieces to the puzzle. This is where a multimodal strategy really proves its worth.
- Somatosensory Evoked Potentials (SSEPs): This test checks if the sensory pathways to the brain are still intact. The bilateral absence of the N20 wave is one of the most specific red flags we have for a devastating neurological injury.
- Biomarkers: Blood tests like Neuron-Specific Enolase (NSE) give us a chemical signal of neuronal damage. If NSE levels are persistently high when measured between 48-72 hours post-arrest, it usually points to more severe brain injury.
- Neuroimaging: A head CT or MRI can show us the structural aftermath. A CT might reveal diffuse cerebral edema (swelling), which looks like a loss of gray-white matter differentiation. An MRI is even more sensitive and can pinpoint specific patterns of anoxic injury.
This comprehensive approach is so important because, while we're getting better, the overall survival numbers for cardiac arrest are still sobering. Even with all our advancements, recent data shows that survival to hospital discharge for shockable rhythms just recently nudged up to 48%. These modest but hard-won gains, highlighted in recent long-term outcome studies, show exactly why meticulous post-arrest care matters so much. It’s how we give every single patient their best shot at a meaningful recovery.
Putting It All Together: Multimodal Neurological Prognostication
No single test tells the whole story. The best approach involves gathering evidence from multiple sources over several days to build a clear and reliable picture of the patient's neurological potential.

By combining these markers, clinicians can make more informed and confident decisions, providing families with a realistic outlook based on a comprehensive evaluation rather than a single, potentially misleading, data point.
Building Expertise Through Modern Education
Let's be honest: navigating these complex evaluations requires sharp, current knowledge. For years, we all relied on in-person weekend courses for things like ACLS certification, which meant dealing with scheduling headaches and taking time away from the unit.
Thankfully, that's changing. The old-school belief that only a handful of legacy organizations like the AHA can provide valid certifications is fading. It's being replaced by a wide acceptance of high-quality online education. In fact, peer-reviewed studies and industry articles consistently show that online learning delivers patient care outcomes and knowledge retention rates that are just as good as—and sometimes even better than—traditional classroom settings.
Hospitals, clinics, and organizations are embracing accredited online certifications because they offer much-needed flexibility, cost savings, and time efficiency without cutting corners on quality. Here at ProMed, our future-focused courses are built for this modern reality. We provide credible, convenient education that equips you with the up-to-date skills you need for complex scenarios like prognostication in care after cardiac arrest.
The Transition to Long-Term Recovery and Rehabilitation
Getting a patient through the initial cardiac arrest is a massive victory, but let's be real—that's just the first leg of the race. The real marathon of care after cardiac arrest starts now, and it's all about managing the fallout and planning for a life beyond the ICU.
The body has just been through a tremendous shock, kicking off a massive inflammatory response called post-arrest syndrome. This often brings myocardial dysfunction along for the ride. Our focus has to shift from crisis mode to a more sustained, supportive approach, looking at everything from the vent settings to where the patient goes after they leave our unit.
Addressing Systemic Complications
Once the dust settles and the patient is stabilized, a whole new set of problems can crop up. Staying one step ahead is the name of the game to prevent secondary issues from derailing their recovery.
- Ventilator Management: Ventilator-associated pneumonia (VAP) is a constant threat. We need to be militant about lung-protective strategies. That means keeping the head of the bed at 30-45 degrees, performing consistent oral care, and working to get them off the vent as soon as it's safe.
- Nutritional Support: The body is burning through calories in a hypermetabolic state. Early nutrition is non-negotiable. Starting enteral feeds within 24-48 hours is crucial to support the gut and give the body the fuel it desperately needs to heal.
- Glycemic Control: Wild blood sugar swings are toxic to an already injured brain. Whether it's hyperglycemia or hypoglycemia, both are bad news. We typically use an insulin drip to keep things in a tight, protective range.
Think of these not as just boxes to check, but as the fundamental building blocks that give the body a fighting chance to repair itself.
The Bridge to Long-Term Rehabilitation
Discharge planning isn't an afterthought; it starts almost immediately. The patient's neurological status is the biggest factor determining their next steps, and this conversation involves the whole team—physicians, nurses, therapists, and case managers.
The numbers paint a stark picture. Out-of-hospital cardiac arrest (OHCA) is a massive public health issue. In the U.S. alone, there are about 356,000 EMS-assessed OHCAs every year. The tough reality is that survival to hospital discharge is only around 10.2%. This is why every single detail of recovery planning matters so much for the people who do survive.
A patient's journey doesn't end at the hospital doors. A well-coordinated discharge plan is essential for bridging the gap between critical care and a patient's new reality, setting them up for the best possible quality of life.
Where a survivor goes after the ICU is completely tailored to their functional and cognitive abilities. The options usually include:
- Long-Term Acute Care Hospital (LTACH): For those who are still medically complex, perhaps even still on a ventilator.
- Inpatient Rehabilitation Facility (IRF): The best fit for patients who can handle several hours of intense physical, occupational, and speech therapy every day.
- Skilled Nursing Facility (SNF): For individuals needing ongoing medical oversight but with less intensive rehab needs.
As they move along their recovery path, encouraging safe physical activity and exercise becomes incredibly important, always customized to their specific condition and cardiac rehab guidelines.
Upholding Modern Educational Standards
Navigating these complex recovery paths demands that we, as healthcare professionals, are constantly learning and adapting. The old way of taking a week off for a stuffy, in-person certification class just doesn't work for most of us anymore.
The entire industry is changing. There's a growing mountain of evidence from peer-reviewed studies showing that high-quality online education is just as effective—in terms of knowledge retention and patient outcomes—as traditional classroom training. Because of this, hospitals and healthcare systems everywhere are embracing accredited online certifications. The old idea that only legacy organizations like the AHA or American Red Cross offer valid credentials is a thing of the past.
ProMed is right there on the leading edge of this shift. We offer accredited online certifications that fit into the reality of a busy clinician's schedule. We give you the essential, current knowledge you need to expertly manage every phase of care after cardiac arrest, from the moment of resuscitation all the way through to long-term recovery planning.
Common Questions About Post Cardiac Arrest Care
Even when you have solid protocols, the bedside reality of post-cardiac arrest care is full of tough calls. Let's dig into some of the common "what ifs" that pop up, moving beyond the algorithm to the real-world decisions that define excellent care.
How Do We Choose a Vasopressor in Complex Cases?
Norepinephrine is the go-to, no question. But what happens when you're dealing with mixed shock states or a patient with a history of serious cardiac problems?
The trick is to match the drug to the patient's specific physiology. If you're looking at profound cardiogenic shock with a severely stunned myocardium, just cranking up the norepinephrine might not be enough. You'll likely need to add an inotrope like dobutamine to give that heart the squeeze it's missing.
On the flip side, what if severe bradycardia is driving the hypotension? In that case, epinephrine might be your best first move for its powerful chronotropic (heart rate) effects.
The best practice here is to get eyes on the heart. A quick bedside echo can tell you more than any blood pressure reading alone. Seeing a poorly contracting ventricle in real-time gives you a clear, actionable target for your therapy.
When Is It Safe to Stop Targeted Temperature Management?
The book says at least 24 hours of cooling, followed by a slow, controlled rewarming. Simple enough. But what if your patient starts waking up and following commands ahead of schedule?
If a patient shows a clear, consistent return of neurological function before that 24-hour mark is up, keeping them deeply sedated and cooled probably isn't doing them any favors. When this happens, it's often reasonable to start the rewarming process early—always with very careful monitoring, of course.
The key word here is clear. You have to be sure you're seeing a true, unambiguous awakening, not just reflexive movements or myoclonus. An early positive neuro change has to be the real deal before you deviate from the standard TTM timeline.
Communicating Prognostic Uncertainty with Families
This is easily one of the hardest parts of the job. How do you give a family hope without sugarcoating a deeply uncertain future?
The most effective way I've found is to frame the conversation around time and the need for multiple data points. You have to explain that the brain takes several days to declare its potential for recovery, and no single test can give us a definitive answer right now.
- Set Clear Timelines: Let the family know you'll be gathering information over the next 72 hours and will share updates as you get them. This manages expectations and gives them a concrete timeframe.
- Explain the "Why": Briefly describe the tools you're using—EEG, clinical exams, imaging—and what each piece of the puzzle tells you about their loved one's brain function.
- Focus on What You Know: Avoid speculation. Stick to the facts. For example, instead of guessing, you can say, "Today, his brain waves are showing some seizure activity, and we are treating that with medication."
This approach builds a foundation of trust. It helps families see that prognostication isn't a snap judgment but a careful, deliberate process.
Keeping up with these complex topics is non-negotiable. The world of medical education has changed, and accredited online certifications are now a standard, accepted way for hospitals and healthcare systems to ensure their staff is up to date. Peer-reviewed studies have confirmed that online learning can provide outcomes on par with traditional in-person training. The outdated belief that only a few specific organizations offer valid credentials is no longer true; the industry is evolving.
ProMed Certifications offers a modern, flexible path to maintaining your credentials, making sure you have the latest, evidence-based knowledge for critical situations like post-cardiac arrest care. Check out our convenient online certification courses at https://promedcert.com.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)
.png)