

Nursing Diagnosis for Asthma: A Complete Clinical Guide
You're at the start of a shift. Your patient is sitting upright, shoulders tense, leaning forward, and working hard to move air. You hear wheezing before you even place your stethoscope. They answer in short phrases, not full sentences. At that moment, “asthma” is only the beginning of your thinking.
The bedside question is more specific. What problem is happening right now, and what does it require from nursing in the next few minutes?
That's why a nursing diagnosis for asthma matters. It translates scattered findings into a clinical priority. It tells you whether your patient mainly needs help clearing the airway, support for oxygenation, coaching to reduce panic, protection from overexertion, or all of those in the right order. Good diagnosis sharpens interventions. It also sharpens documentation, handoff, and escalation.
Asthma can change quickly. A patient may start with tight airways and mild distress, then slide into poor gas exchange or exhaustion if subtle warning signs are missed. That's where strong nursing judgment shows up. You're not just matching symptoms to a label. You're reading patterns, spotting drift, and acting before deterioration becomes obvious.
Your Guide to Nursing Diagnosis for Asthma
A new nurse often asks, “How do I know which diagnosis fits best when everything seems respiratory?” The answer starts with the patient in front of you.
Take a common scenario. Your patient says, “I can't get a deep breath.” You hear diffuse wheezing. Their cough is frequent but not productive. They look frightened. If your first thought is ineffective airway clearance, that's reasonable. If their oxygenation starts slipping, restlessness increases, and their color changes, your priority may shift to impaired gas exchange.
What the diagnosis is really doing
A nursing diagnosis for asthma isn't a paperwork exercise. It's a way to organize bedside reality.
Consider it triage inside your own care plan:
- Airway problem means air is struggling to move through narrowed, mucus-filled passages.
- Gas exchange problem means oxygen and carbon dioxide aren't moving well at the lung level.
- Breathing pattern problem means the mechanics of breathing are off.
- Anxiety problem means fear is amplifying distress and making self-management harder.
- Activity problem means even small tasks push the patient past their respiratory reserve.
When nurses confuse those categories, care becomes vague. When nurses separate them clearly, care becomes focused.
Clinical shortcut: Ask yourself, “What's the biggest immediate threat. Air movement, oxygenation, breathing effort, or the patient's ability to participate in care?”
What you'll see at the bedside
Most asthma patients won't present as textbook examples. They overlap.
You may see:
- The talkative patient who suddenly goes quiet because breathing now takes more effort.
- The anxious adolescent who reaches for a rescue inhaler repeatedly, but can't explain trigger patterns.
- The older adult whose wheeze is less obvious than their fatigue and rising work of breathing.
Your diagnosis has to match the current state, not the chart history.
That's also why modern asthma care rewards nurses who think dynamically. The strongest clinicians don't just identify what is happening. They notice what is about to happen.
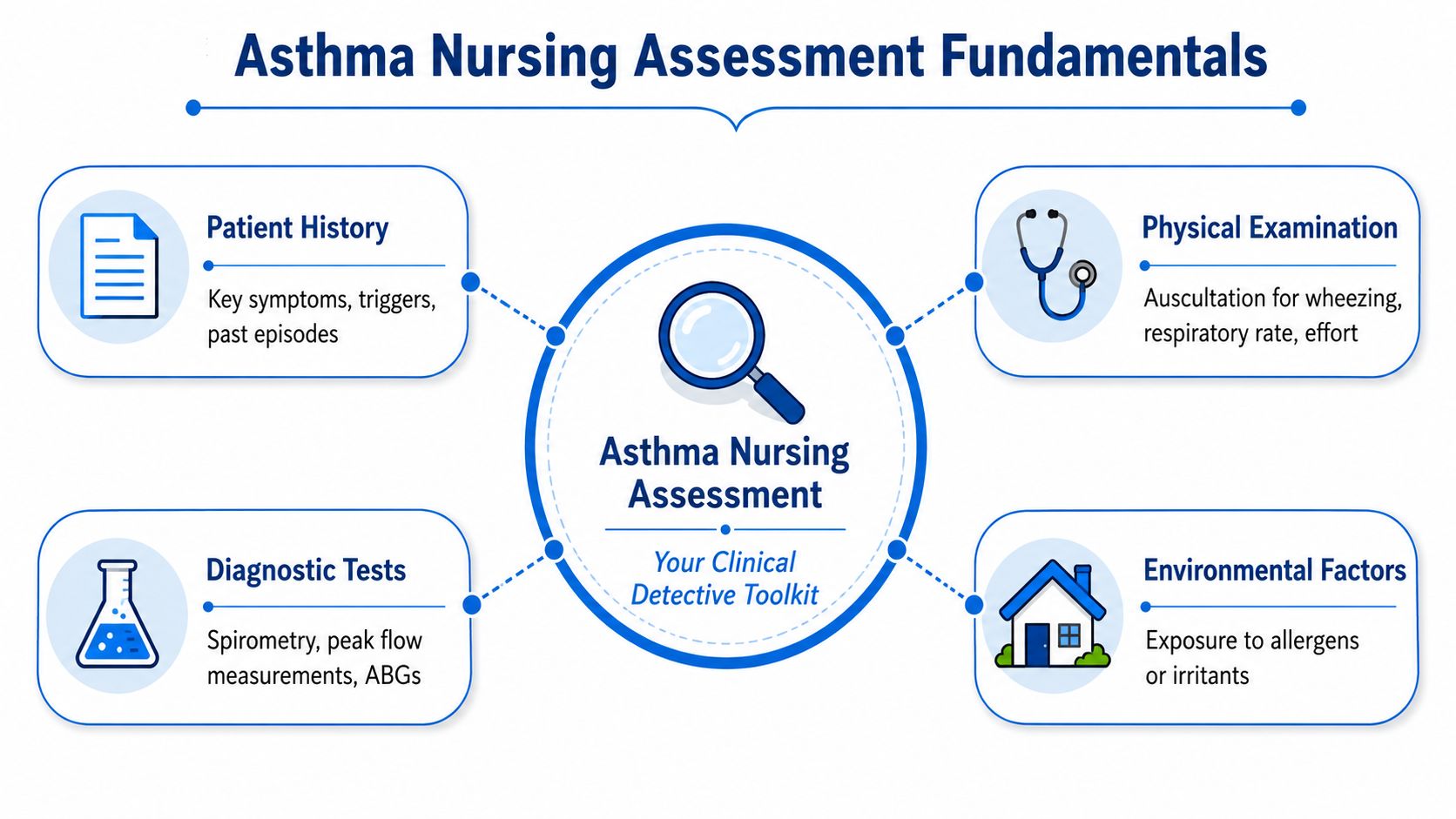
Asthma Nursing Assessment Fundamentals
Before you write any diagnosis, gather evidence like a clinician building a case. Asthma assessment has moved far beyond “patient is wheezing.” A 2024 review reports worldwide asthma prevalence of 9.1% in children, 11% in adolescents, and 6.6% in adults, and notes that nursing assessment commonly includes BMI, vital signs, peak expiratory flow, inhaler-technique verification, and Asthma Control Test screening as part of structured control monitoring in practice (PMC review on global asthma prevalence and assessment).
Start with what you can see and hear
Walk into the room and assess before touching anything.
Notice:
- Work of breathing. Is the patient using accessory muscles, leaning forward, or struggling to finish sentences?
- Respiratory rate and pattern. Fast breathing matters, but so does shallow breathing or prolonged exhalation.
- Auscultation findings. Wheezing is common, but diminished breath sounds can be more ominous because they may suggest poor airflow.
- Color and mentation. Restlessness, agitation, or confusion may be early signs that oxygen delivery is worsening.
Add objective tools
Assessment gets stronger when you pair observation with measurement.
Use:
- Pulse oximetry to trend oxygenation in real time
- Peak expiratory flow when the patient can perform it reliably
- Asthma Control Test screening in non-emergent settings
- Inhaler-technique verification because poor technique often explains poor control
- Vital signs as a pattern, not isolated numbers
A good asthma assessment is like checking both the weather and the radar. Symptoms tell you what the patient feels. Objective measures tell you where the storm is heading.
Don't skip the history that changes care
Ask about triggers, recent exposure, prior severe episodes, home meds, and what the patient did before arriving. Environmental irritants, adherence problems, and incorrect inhaler use often explain why a patient isn't responding as expected.
For nurses maintaining competency in these assessment skills, ProMed+ Nursing CE is one example of an online CE platform. ProMed+ is your ultimate one-stop shop for all continuing education needs. Easily fulfill every CE requirement with our exceptional streaming platform.
Primary Diagnosis Ineffective Airway Clearance
Ineffective airway clearance is often the first nursing diagnosis for asthma because the immediate problem is narrowed airways filled with inflammation and mucus. The patient may be moving air poorly, coughing without relief, and describing chest tightness or the sense that air won't go in all the way.
How to recognize it
This diagnosis fits when the airway itself is the main issue.
Common clues include:
- Audible wheezing
- Persistent cough, often not very productive
- Prolonged expiratory phase
- Tight chest and difficulty taking a full breath
- Accessory muscle use when effort increases
- Diminished tolerance for talking or activity
Students often encounter difficulty here. Wheezing alone doesn't tell you everything. Ask whether the patient is moving air effectively. A loud wheeze can be concerning, but a suddenly quieter chest in a tiring patient can be worse.
What current practice looks like
Nursing references identify spirometry as the preferred diagnostic test for asthma and recommend gauging severity before treatment. For unstable patients, respiratory and vital-sign checks are often performed every four hours or more frequently, which helps guide bronchodilators, suctioning, and other interventions to prevent hypoxia.
That bedside pattern matters. You assess, intervene, reassess, and compare trends. Asthma doesn't reward one-time checks.
Prioritized interventions that make sense
Think in terms of opening space and reducing the patient's workload.
- Position first. High-Fowler's usually helps lung expansion and reduces the effort of breathing.
- Give bronchodilators as ordered. These target bronchospasm, which is one of the main reasons airflow is restricted.
- Encourage fluids if appropriate. Hydration can help keep secretions from becoming thicker and harder to move.
- Coach breathing and coughing. A patient in distress may need direct, calm instruction to slow down and cough effectively.
- Reduce triggers in the room. Smoke exposure, strong scents, dust, and cold air can all worsen symptoms.
- Suction if needed and ordered. Not every asthma patient needs it, but some do when secretions are contributing to obstruction.
Don't document “airway clearance improving” unless you can tie it to findings such as easier speech, reduced wheezing, better cough effectiveness, or less visible work of breathing.
A practical outcome statement might read: patient maintains more effective airflow, demonstrates less labored breathing, and shows improved breath sounds during the shift.
If the patient deteriorates and you begin thinking about advanced airway support, it helps to review airway adjunct options such as laryngeal mask airway placement basics.
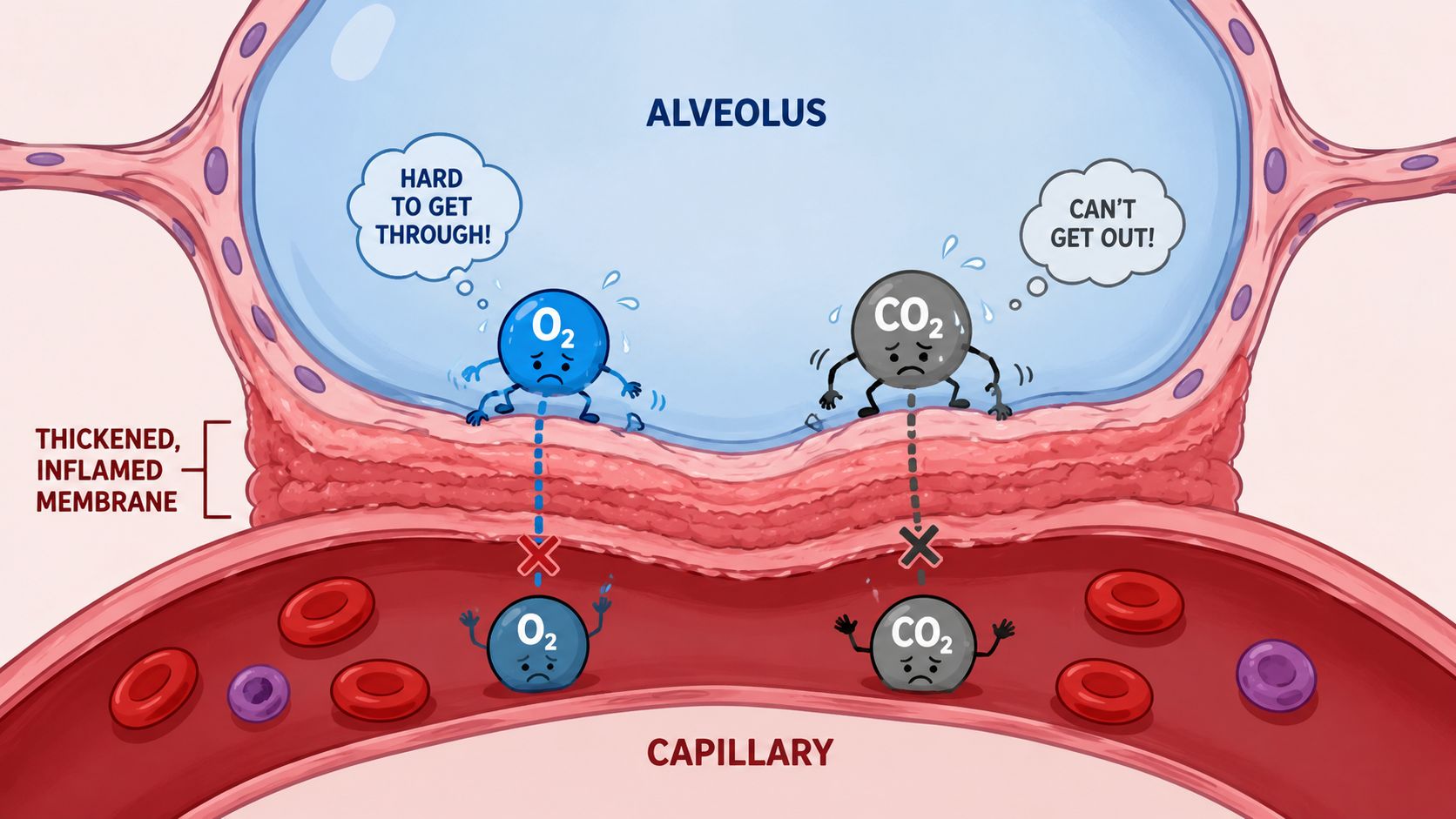
Critical Diagnosis Impaired Gas Exchange
Impaired gas exchange is more urgent than simple airway obstruction because now the problem has reached oxygen and carbon dioxide transfer. In asthma, worsening bronchospasm and mucus plugging can create enough ventilation mismatch that the patient isn't oxygenating well or begins retaining carbon dioxide.
When this becomes your top priority
This diagnosis should move to the front when your findings suggest oxygenation failure, not just tight airways.
Key warning signs include:
- Dropping oxygen saturation
- Restlessness or confusion
- Cyanosis
- Increasing fatigue
- Less effective ventilation despite treatment
A high-acuity asthma diagnosis needs high-acuity thinking. The patient may still be wheezing, but the real question is whether gas exchange is holding.
According to a nursing care reference, SpO2 below 90% is a critical warning threshold in asthma. Pulse oximetry is used for early detection, and ABGs become important when oxygenation isn't restored above that level or when you suspect respiratory acidosis from hypoventilation (Nurseslabs asthma care plans).
Airway problem versus gas exchange problem
A simple comparison helps:

This difference is easy to miss when you're busy. Many patients have both. Your job is to identify which one is driving immediate risk.
What you do next
When impaired gas exchange is present, your nursing actions become more vigilant.
- Apply oxygen as ordered and evaluate whether it's helping.
- Use continuous pulse oximetry when the patient is unstable.
- Prepare for ABGs if oxygenation doesn't improve or the patient looks more exhausted.
- Reassess mental status often because subtle confusion can be an early sign of worsening hypoxia.
- Escalate quickly when the patient is tiring, less responsive, or failing to improve.
If your patient's oxygenation is dropping and their effort is rising, don't let a familiar asthma label make the situation feel routine.
A helpful companion concept is the difference between distress and failure. This overview of respiratory distress vs respiratory failure can help clarify when your patient has crossed into a more dangerous phase.
Anxiety and Activity Intolerance in Asthma
Asthma doesn't stay confined to the lungs. It changes how patients think, move, and respond to symptoms. Two common nursing diagnoses that often accompany the respiratory problem are anxiety and activity intolerance.
Anxiety is not always “just anxiety”
Breathlessness is frightening. Patients may become restless, panicked, or unable to focus on instructions. Some hyperventilate from fear on top of airway narrowing, which can make the whole episode feel even worse.
Your assessment should look for:
- Verbalized fear, such as “I'm going to stop breathing”
- Restlessness or agitation
- Difficulty following coaching
- Escalating distress out of proportion to exam findings
- Reliance on rescue behaviors that don't match the care plan
Supportive nursing care matters here. Calm voice, short directions, breathing coaching, and staying physically present can reduce spiraling fear. Pursed-lip breathing and paced coaching can give the patient a sense of control while medical treatment is working.
Asthma-specific catastrophizing
There's a more nuanced pattern nurses should watch for. Some patients' anxiety is more intense. They interpret any wheeze or chest sensation as proof that death is imminent. That can lead to overuse of rescue medication at times, and dangerous delay at others because fear makes thinking less organized.
Recent 2025 data report that 42% of adolescent asthma patients with high Asthma-Specific Catastrophizing scores were misdiagnosed with standard anxiety, and that this was associated with a 3.5x higher hospitalization rate when targeted cognitive interventions were not used.
That finding matters clinically. If you treat every fearful asthma patient as having generic anxiety, you may miss a pattern that directly affects adherence, self-monitoring, and when the patient seeks help.
Some patients need reassurance. Others need structured teaching that separates “I feel a symptom” from “I am in immediate danger.”
Activity intolerance shows up in small tasks
Patients with asthma often don't complain first about “activity intolerance.” They say they're too winded to walk to the bathroom, talk while standing, or finish routine tasks.
Look for:
- Dyspnea with mild exertion
- Need for frequent pauses
- Visible fatigue after basic care
- Worsening respiratory effort during activity
- Reduced willingness to move because symptoms flare
A simple bedside approach works well:
- Assess response before activity.
- Watch breathing effort during the task.
- Reassess recovery afterward.
Then plan care around what the patient can tolerate. Cluster tasks. Allow rest. Reduce unnecessary exertion during acute symptoms. As the patient stabilizes, encourage gradual return to activity instead of pushing too hard too soon.
Building an Effective Asthma Nursing Care Plan
A strong care plan for asthma isn't a list of problems. It's a priority map. You decide what can wait and what can't.
A 2024 study reported that 68% of acute asthma exacerbations leading to ICU admission involved a missed window where early nursing indicators were not weighted in predictive triage models. The point for practice is simple. Small findings matter when they cluster. Subtle oxygen dips, slight increase in accessory muscle use, and a patient who suddenly can't speak as easily may be early signs of a larger decline.
Start with the highest-risk diagnosis
If your patient has both wheezing and poor oxygenation, impaired gas exchange comes before activity intolerance. If the patient is oxygenating adequately but struggling to move air through inflamed bronchi, ineffective airway clearance may lead.
A simple bedside example
Consider a patient with wheezing, accessory muscle use, rising anxiety, and falling oxygen saturation.
Your prioritized plan might look like this:
- Impaired gas exchange
- Outcome: patient shows improving oxygenation and reduced signs of hypoxia
- Interventions: oxygen as ordered, continuous pulse oximetry, close reassessment, escalation if worsening
- Ineffective airway clearance
- Outcome: patient demonstrates easier airflow and less labored breathing
- Interventions: positioning, bronchodilator administration, trigger reduction, cough support, reassessment
- Anxiety
- Outcome: patient verbalizes reduced panic and follows breathing instructions more effectively
- Interventions: brief explanations, calm presence, paced breathing coaching, reassurance grounded in current findings
- Activity intolerance
- Outcome: patient completes necessary activity with manageable symptoms
- Interventions: rest periods, clustered care, progressive activity as tolerated
- What you assessed. Breath sounds, work of breathing, ability to speak, oxygenation trend, anxiety cues.
- What you did. Positioning, oxygen, bronchodilator administration, education, escalation.
- How the patient responded. Easier speech, decreased wheeze, improved oxygenation, persistent distress, new fatigue.
- Trigger recognition. Help them identify what reliably worsens symptoms at home, work, school, or outdoors.
- Inhaler and spacer technique. Many patients think they know how to use them, but return demonstration often shows gaps.
- Action planning. They need to know what to do when symptoms begin, when home steps are no longer enough, and when emergency care is necessary.
- Teach-back. Ask the patient to explain the plan in their own words.
Documentation that actually helps
Good charting tells the patient's respiratory story clearly.
Document:
This becomes even more important when you're acting on subtle trends. If you want a practical bedside framework for response priorities, this guide to asthma attack nursing interventions is a useful companion read.
Online CE is especially valuable here because predictive assessment is easier to learn when you can revisit scenarios, pause, and review pattern recognition on your own schedule. For CE and certifications, online learning is a valid format and healthcare institutions increasingly recognize that it can support the same clinical judgment skills nurses use in person.
Patient Education and Empowering Lifelong Management
A patient can leave the unit breathing easier and still be headed for another exacerbation if education is weak. That's why knowledge deficit often becomes the discharge-phase nursing diagnosis that matters most.
What patients need to understand before discharge
Keep teaching practical. Patients usually remember actions better than lectures.
Focus on:
Environmental control deserves plain-language teaching too. If a patient connects respiratory flares with indoor irritants, practical home discussions help. For example, when families ask about dust and allergen buildup, I'll sometimes share educational reading on air duct cleaning for allergies as one part of a broader conversation about the home environment.
Why ongoing professional education matters
Patient teaching improves when clinicians stay current. Asthma care changes, inhaler devices change, and our understanding of risk signals keeps evolving.
That's one reason online CE and certifications matter so much for working clinicians. They're not a lesser substitute for classroom learning. For many nurses, they're a more realistic way to review, repeat, and retain material while balancing shifts and family life. The old idea that only in-person AHA or Red Cross formats are valid no longer matches the way many healthcare professionals maintain competency. High-quality online education is widely used, increasingly accepted, and well suited to adult learners who need flexibility without sacrificing rigor.
If you want to build stronger respiratory assessment, documentation, and emergency response skills, ProMed Certifications offers online medical certification courses for healthcare professionals, including ACLS, PALS, BLS, Neonatal Resuscitation, and CPR.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)
.png)