Cultural Competency CME: Your 2026 Guide to Requirements

You open your inbox between patients and see it. A notice from your licensing board, credentialing office, or employer says you need cultural competency CME. Your first reaction might be predictable: one more requirement, one more certificate, one more hour you don't have.
That reaction makes sense. Most clinicians already juggle clinical volume, inbox work, documentation, renewals, and mandatory training that often feels disconnected from day-to-day care.
But this topic is worth treating differently. Done well, cultural competency education isn't about memorizing labels or trying to become an expert in every community you serve. It's about improving the clinical skills you already use: listening, explaining, checking understanding, building trust, and adjusting your approach when a patient's beliefs, language, family structure, or past healthcare experiences shape the encounter.
It also doesn't have to disrupt your schedule. Accredited online CME has made compliance much easier for busy professionals. In practice, many clinicians now complete these requirements the same way they complete other modern CE activities: on demand, on their own time, with documentation ready when they need it.
The New Requirement on Your CME List
A typical version of this goes like this. You're reviewing renewal tasks late in the evening. DEA training is on the list. Your specialty CME is still incomplete. Then you notice a board-specific requirement for cultural competency, implicit bias, or related equity training.
Your first question usually isn't philosophical. It's practical. What exactly do I need, and what counts?
That's the right question.
Some clinicians assume this requirement is mostly symbolic. Others worry it means sitting through a long in-person class that won't help them in clinic. Neither assumption is very useful. The better approach is to treat it like any other licensure task: verify the rule, choose an accredited course, finish it efficiently, and keep the certificate.
Practical rule: Don't start with a course catalog. Start with your own licensing board, certifying body, employer policy, or credentialing office.
The confusion often comes from the label itself. One board may call it cultural competency. Another may group it with implicit bias, health equity, patient communication, or disparities training. The wording changes, but the compliance task is similar. You need education that fits the requirement and comes from a provider your board accepts.
A lot of clinicians also still assume only classroom training “really counts.” That's outdated. For CME and CE, accredited online education is a standard path to compliance across healthcare. If the provider is properly accredited and the activity meets your board's rule, the fact that you completed it online doesn't make it lesser.
What busy clinicians usually need most
Individuals don't need a lecture on why forms exist. They need a short decision process:
- Check the exact requirement: Look for hour count, topic wording, renewal cycle, and whether it's one-time or recurring.
- Confirm accepted accreditation: For physicians, nurses, pharmacists, and other licensed professionals, accepted accrediting bodies matter.
- Choose format strategically: If your schedule is fragmented, online self-paced education is often the simplest option.
- Save proof immediately: Download the certificate and store it where you keep your license and renewal records.
That's the no-nonsense approach. It keeps the task small, and it keeps you compliant.
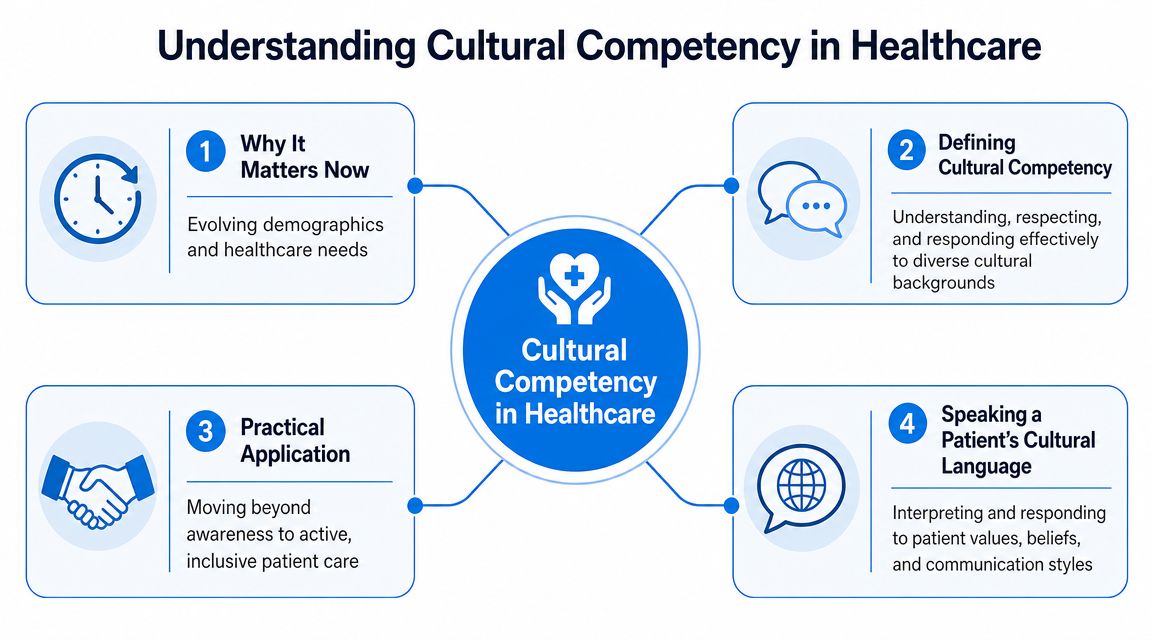
What Is Cultural Competency in Healthcare
At its most practical, cultural competency in healthcare means giving care that is respectful, understandable, and responsive to patients whose backgrounds, values, beliefs, communication styles, or life circumstances differ from your own.
Think of it as learning part of a patient's cultural language. Not their spoken language alone, though that matters too. Their cultural language includes what illness means to them, who helps make decisions, what they fear, what they trust, and how they interpret your recommendations.
What it is and what it isn't
Many people misunderstand this concept. Cultural competency does not mean:
- Memorizing stereotypes: No course should teach that all members of any group think or act the same way.
- Performing perfect language: You don't need to say everything flawlessly to provide respectful care.
- Replacing clinical judgment: Clinical standards still matter. The goal is to communicate and apply them more effectively.
It does mean strengthening a few core habits:
- Self-awareness: noticing your assumptions before they affect the visit
- Curiosity: asking rather than assuming
- Communication skill: explaining plans in ways patients can use
- Adaptability: adjusting care discussions to the person in front of you
A recent scoping review found that reported cultural competence levels among healthcare professionals were mostly moderate or low, and few studies tested training interventions, which supports the need for education focused on real-world care rather than simple completion scores, as described in this scoping review of cultural competence in healthcare professionals.
What shows up in a typical course
Most cultural competency CME activities cover a mix of clinical communication and systems awareness. Common topics include:
- Implicit bias: how automatic assumptions can affect listening, diagnosis, and recommendations
- Health literacy: whether patients can understand and act on the plan you gave them
- Social determinants of health: factors outside the exam room that shape what is realistic
- Inclusive communication: language that avoids alienating or confusing patients
- Working with interpreters: how to improve accuracy, empathy, and patient engagement
- Respect for decision-making context: including family roles, faith, identity, and prior healthcare experiences
How this looks in practice
A clinician tells a patient to return in two weeks, start a new medication, and avoid certain foods. The patient nods, then doesn't follow through. It's easy to call that nonadherence.
A culturally competent approach pauses before making that judgment. Did the patient understand the plan? Can they afford the medication? Does fasting for religious reasons affect the schedule? Is a family member involved in decisions? Did shame, mistrust, or language barriers block questions?
Those aren't abstract concerns. They're routine clinical realities.
Good cultural competency training helps you ask better questions before you label the outcome.
Why This Training Is Critical for Patient Outcomes
A patient agrees to the plan, leaves the visit, and never starts the medication. The chart can make that look like simple nonadherence. In real practice, the gap is often more basic. The instructions were unclear, the family decision-maker was not in the room, the patient did not trust the recommendation, or the plan collided with daily life in ways no one addressed.
That is where cultural competency CME earns its place on an already crowded CME list. It helps clinicians reduce avoidable friction in care. The immediate target is not ideology. It is better history-taking, clearer communication, stronger trust, and plans patients can implement.
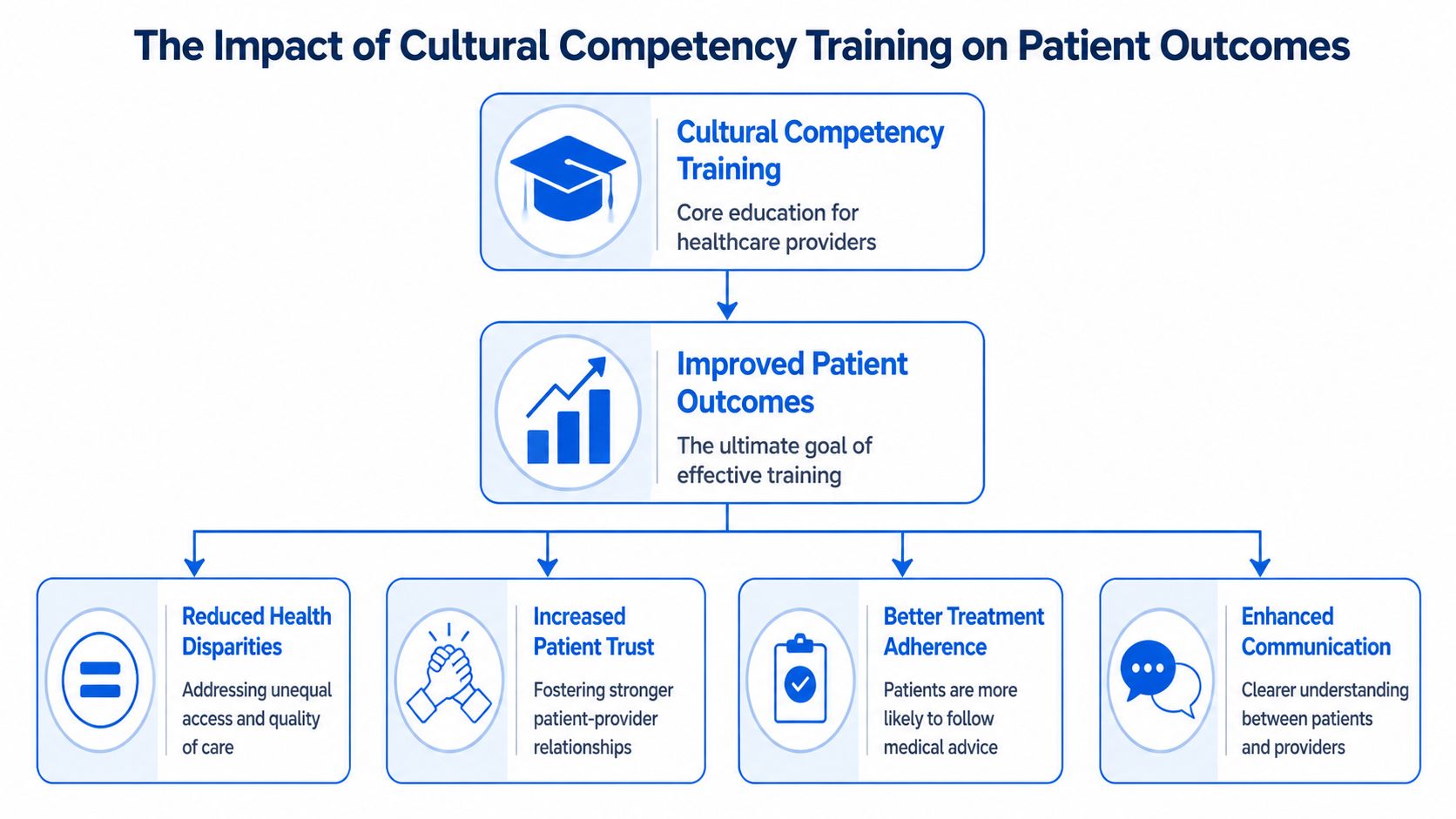
What the evidence supports clearly
A 2011 systematic review of 34 studies on cultural competence training found a consistent pattern. Training improved clinician knowledge, attitudes, and skills. That last point matters most to a busy clinician, because skills are what show up in the exam room.
Skills training works like adjusting the focus on a lens. The patient was always giving you information, but you may not have been seeing the barriers clearly. A better question, a better interpreter workflow, or a more careful explanation can change the whole encounter.
Where the evidence is more limited
Patient outcomes are harder to measure than learner outcomes. They also depend on factors no single course can fix, including transportation, cost, staffing, interpreter access, and prior experiences with the health system.
So the realistic standard is not, "Will one CME module solve disparities?" It will not. The better question is, "Will this training help me make fewer avoidable mistakes in communication and decision-making?" In many cases, yes.
That is an important distinction.
Why it matters in daily care
You have probably seen this already without calling it cultural competency. A patient with low health literacy says "yes" to everything, then goes home confused. An older adult defers to a daughter who was never included in the discussion. A patient declines a test because prior care felt dismissive, not because they "do not care." The clinical problem and the communication problem arrive together.
Maternity care offers a clear example. Conflicts can build when the patient, physician, and support team enter the room with different expectations about autonomy, safety, and who gets a voice. Bornbir's discussion of doula physician conflict shows how quickly role confusion and mismatched assumptions can disrupt care that should have been collaborative.
The practical value of this training is simple. It helps you slow down at the right moment, ask one better question, and test whether the plan fits the patient in front of you. That is not compliance theater. It is clinical efficiency, because preventable misunderstanding costs time, follow-up, and trust.
For clinicians who hold nursing credentials or work in mixed-discipline teams, state-specific continuing education requirements for nurses by state also show how often communication and equity topics are being tied to licensure expectations.
The useful test for any cultural competency course is straightforward. Does it change what you do with the next patient you see?
The strongest courses leave you with habits you can use immediately. Use plain language. Ask who helps make decisions at home. Check understanding without shaming the patient. Notice when mistrust, language, or prior harm may be shaping the visit. Those small adjustments are often the difference between a plan that is documented and a plan that is followed.
Navigating State and Board CME Mandates
Requirements vary enough that guessing is risky. One state may require a specific topic during each renewal cycle. Another may require a one-time course. An employer may add its own annual training on top of licensure rules. If you hold multiple licenses, the overlap can get messy fast.
The practical answer is simple. Read the exact rule that applies to your license.
A 2020 national physician survey published in Family Medicine helps explain why these mandates have expanded. In that nationally representative weighted sample of 290,109 physicians, 66.3% reported receiving cultural competence training at some point, but only 18.7% said it was required for newly hired physicians in their practice, and only 34.5% of those who had any training had completed it within the prior 12 months. The same study found that 35.5% had ever heard of the CLAS standards.
The kinds of rules you're likely to see
You don't need a list of every jurisdiction to understand the pattern. Most mandates fall into a few categories:
- Renewal-cycle requirement: complete the course during each licensure period
- One-time requirement: finish it once, then retain documentation
- Topic-specific requirement: the rule may name cultural competency, implicit bias, disparities, or equity-related education
- Role-specific requirement: physicians, nurses, and other disciplines may face different wording or approval standards
How to verify that a course will count
People waste time when they choose a course first and verify second.
A faster approach is to check these items before you enroll:

For nurses managing varying rules across jurisdictions, this overview of continuing education requirements for nurses by state is a useful starting point before checking the official board page.
What accreditation labels usually mean
You'll commonly see acronyms such as ACCME, ANCC, and ACPE on CME and CE sites. The exact relevance depends on your profession, but the main point is straightforward. Recognized accreditation tells you the provider isn't just issuing a certificate. It indicates the activity is being offered through a framework boards and institutions are more likely to accept.
If a provider makes it hard to find accreditation details, move on.
That one step prevents most compliance mistakes.
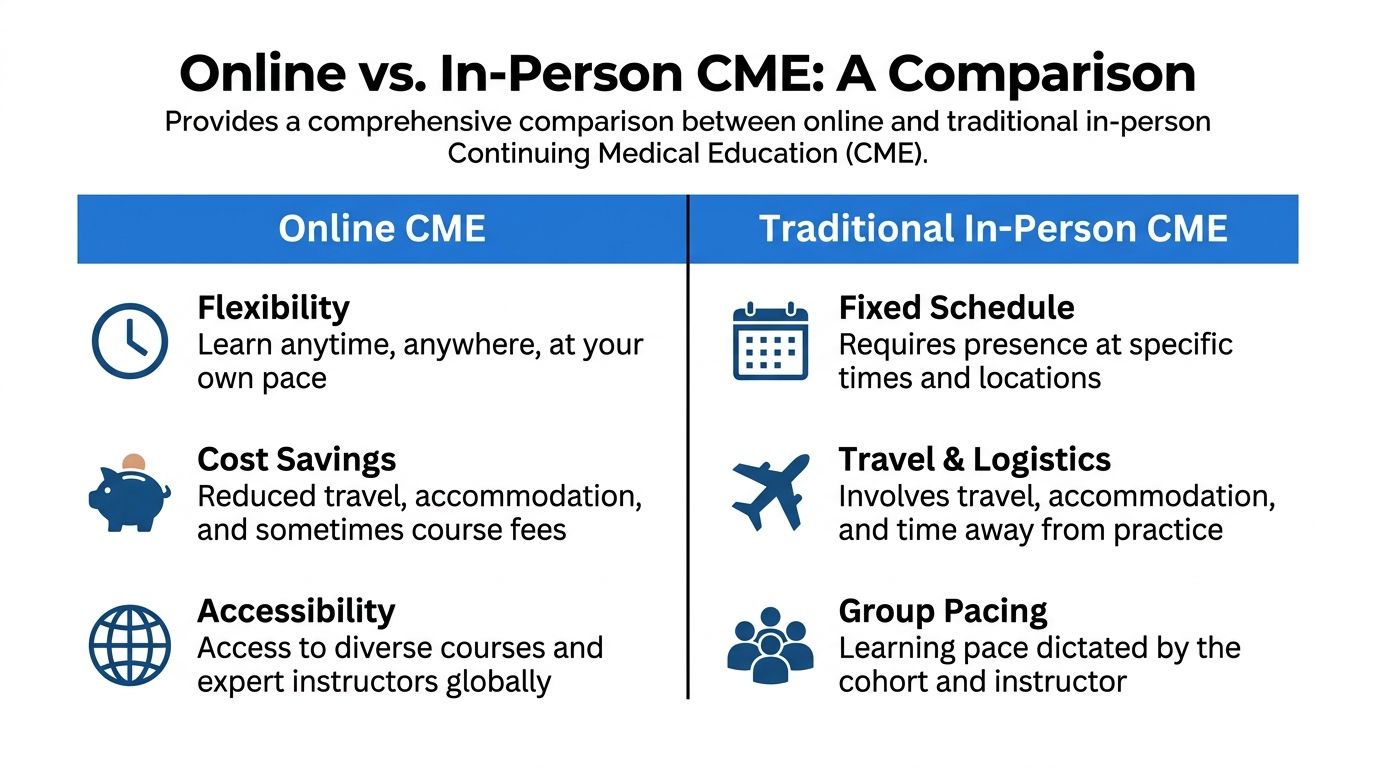
The Clear Advantages of Online CME
For most clinicians, the best format is the one they'll complete on time. That's one reason online CME has become such a practical fit for cultural competency training.
The old assumption that in-person education is automatically better doesn't hold up well in everyday professional learning. For many CE activities, what matters is accreditation, content quality, relevance, and whether the format lets you engage with the material without derailing your schedule.
Why online works well for this topic
Cultural competency CME is especially well suited to online delivery because much of the learning involves reflection, case-based judgment, communication choices, and scenario review. Those activities don't require a hotel ballroom.
Online formats also help in ways clinicians feel immediately:
- Flexible timing: complete a module after clinic, on a day off, or in short sessions
- Less logistical friction: no travel, parking, room schedules, or time away from patients
- Repeat access: revisit a section if a concept didn't land the first time
- Faster documentation: certificates are typically available right away
The in-person myth that still lingers
Some clinicians still hear versions of the same claim: only certain major organizations or classroom-based programs are valid. That's not how continuing education works in most real-world compliance settings.
What counts is whether the activity is accredited, matches your requirement, and is accepted by the relevant board or institution. Online education is widely used across healthcare for CME, CE, and certification-related learning. The format itself is not a disqualifier.
That matters for busy professionals because online learning isn't a compromise. It's often the most realistic way to complete training carefully instead of rushing through a fixed-time event.
A simple comparison

If a course is accredited and relevant to your requirement, online completion is a legitimate professional choice, not a lesser one.
That's the practical standard most clinicians should use.
How to Select a High-Quality Online Course
You are on a licensing deadline, you find a one-hour course that looks convenient, and one question decides whether that hour solves the problem or creates another one later. Will this course count, and will it prove helpful in clinic?
That is the right way to screen online cultural competency CME. Start with compliance. Then look at educational quality. In practice, the best course does both.
The first screen is accreditation
Accreditation is the course's passport. Without it, a polished website and a fast certificate may not mean much.
You should be able to confirm three things within a minute or two. Who accredits the activity. What credit type is offered. Whether the course description clearly fits your profession and requirement. If you want a practical overview of how self-paced training is evaluated, this guide to continuing medical education online is a useful reference.
A credible provider makes this easy to verify. If you have to hunt through FAQs, checkout pages, or fine print to find accreditor information, slow down and check more carefully.
Choose training that teaches behavior, not just terminology
A good course does more than define bias, culture, or disparity. It shows what those ideas look like during a real visit.
That matters because cultural competency is applied work. It shows up when a patient nods politely but does not understand the plan, when family decision-making affects consent, or when an interpreter should have been brought in five minutes earlier. The stronger courses teach clinicians what to say, what to ask, and what to change.
A course is usually stronger if it includes:
- Case-based scenarios: patient encounters that resemble real clinical decisions
- Communication examples: wording for sensitive questions and moments of misunderstanding
- Reflection prompts: brief exercises that help you notice habits that affect care
- Practice tools: interpreter use, health literacy checks, inclusive history-taking, and family communication
A weaker course often stays at the slogan level. You get broad statements about respect and diversity, then a short quiz with little connection to daily practice.
Questions to ask before you enroll
Use a short screening checklist and be literal about it:
- Is the accreditor named clearly on the course page?
- Does the topic wording match your board, employer, or credentialing rule?
- Are the learning objectives specific enough to predict what you will learn?
- Does the course explain how the content applies in patient care?
- Will you get a certificate immediately, and can you download it later if needed?
One practical tip helps avoid headaches. Read the course page the way an auditor would read it. If the activity description is vague to you now, it may be hard to defend later.
Red flags that deserve skepticism
A few warning signs come up often:
- No visible accreditor information
- No instructor, author, or editorial review listed
- No meaningful learning objectives
- No sign of current clinical application
- Marketing that emphasizes the certificate more than the teaching
Choose the course that makes your next patient conversation clearer, while also meeting the rule you need to satisfy.
That standard is simple, efficient, and usually accurate.
Your Action Plan for Completing Cultural Competency CME
If this requirement has been sitting on your to-do list because it felt vague or annoying, reduce it to a short workflow. That's usually all it takes.
A five-step plan that works
- Verify your rule
- Check your licensing board, employer, or credentialing body. Confirm the topic wording, frequency, and whether the activity must come from a specific type of provider.
- Choose an accredited online provider
- Don't assume all certificates are equal. Confirm that the course offers credit through recognized accreditation and fits your profession.
- Pick a course with usable content
- Prioritize training that includes practical communication skills, case examples, and patient-centered application. You're more likely to retain it, and it's more likely to help in clinic.
- Complete it on your schedule
- Online learning makes this easier. You can finish the activity in one sitting or break it up around shifts and call responsibilities.
- Save and report your documentation
- Download the certificate immediately. Store it with your renewal records. If your board requires self-reporting, do it the same day so the task is fully closed.
Common points of confusion
Clinicians often ask whether one course will count everywhere. Sometimes it will. Sometimes it won't. Acceptance depends on your profession, board, and the wording of the requirement. That's why verification comes first.
Another common question is whether online completion is acceptable. In many CME and CE settings, yes. The deciding factors are the course's accreditation and your board's rules, not whether you sat in a classroom.
For clinicians looking to simplify the rest of their annual education strategy, this roundup of 8 ways to earn CME credits can help you bundle requirements more efficiently.
Keep the standard simple
Use this test when you're deciding whether a course is worth your time:
- Will my board accept it?
- Can I complete it without disrupting patient care?
- Will it give me a better way to communicate in difficult visits?
If the answer is yes to all three, you've found the right fit.
The best cultural competency CME is efficient to complete, easy to document, and immediately useful in practice.
You don't need to overcomplicate this. Verify the requirement, choose well, finish it, and move on with one more important item handled professionally.
If you want an easier way to complete accredited online education on your schedule, ProMed Certifications offers a modern path for busy healthcare professionals. Their platform is built for self-paced learning, quick certificate access, and practical compliance across CME, CE, and certification needs.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)