What Is a Utilization Review Nurse?

A utilization review nurse is a registered nurse who reviews patient records, treatment plans, and documentation to decide whether care is medically necessary, appropriate, and cost-effective. Most employers expect 2 to 5 years of acute-care RN experience, and reported U.S. pay has included an average of $79,456 in August 2022 and a 2023 median around $89,700.
If you're a nurse who still loves clinical thinking but feels ready to step away from the bedside, this role often comes up for good reason. It lets you use your assessment skills, documentation judgment, and understanding of patient care in a non-bedside path that still has real impact on treatment, reimbursement, and care coordination.
Your Next Step in Nursing Might Be Off the Floor
A lot of nurses reach a point where they want something different, not because they care less, but because they want a role that uses their experience in a new way. Maybe you want more predictable hours. Maybe you enjoy chart review, problem-solving, and seeing the bigger system around patient care. That's where utilization review can make sense.
A utilization review nurse, often called a UR nurse, sits in a key spot between bedside care, insurance requirements, and hospital operations. You're looking at whether a service, admission, procedure, or continued stay meets the standards for medical necessity and reimbursement. That sounds administrative on paper, but in real life it's still highly clinical.
Why experienced nurses fit this role
This isn't usually an entry-level RN job. Employers commonly expect 2 to 5 years of acute-care RN experience, because the work depends on solid clinical judgment and the ability to recognize what's normal, what's urgent, and what documentation is missing, as noted by the American Nurses Association overview of utilization management nursing.
That same nursing resource also notes reported pay figures that show the specialty's value, including an average annual pay of $79,456 in August 2022 and a 2023 U.S. median around $89,700 in industry salary reporting.
If you're exploring where nursing can take you next, it helps to look at the broader range of career options for registered nurses. Utilization review stands out for nurses who like clinical detail, interdisciplinary communication, and work that affects both patient access and organizational outcomes.
The nurses who often transition well into UR are the ones who already ask, “Does this chart tell the full story?”
What makes this path different
UR nursing is a non-bedside role, but it isn't detached from patient care. Your decisions and recommendations can influence whether a patient stays inpatient, moves to a different level of care, gets a service approved, or needs stronger documentation before a payer will authorize treatment.
That's why many nurses describe the role as part investigator, part advocate, and part translator. You're translating clinical facts into the language that payers and health systems use to make coverage decisions.
The Core Mission of a Utilization Review Nurse
At its center, utilization review is about one question. Does the documented care support the medical necessity of what's being ordered or provided?
That sounds simple until you're applying it to real charts. A patient may clearly look sick to the bedside team, but if the chart doesn't show the needed findings, treatment intensity, or failed lower-level options, the case may not meet payer criteria on paper. That gap is where UR nurses work.
The bridge between care and coverage
A utilization review nurse performs evidence-based chart review to determine whether an admission, procedure, or continued stay meets medical-necessity criteria, often using payer rules and clinical guidelines such as MCG or InterQual, as described in this Nurse.com explanation of utilization review nursing.
It functions as quality control for healthcare decisions, emphasizing clinical judgment. You aren't just checking whether forms are complete. You're reviewing the story the chart tells.
That often means asking questions like these:
- Admission level: Does this patient meet inpatient criteria, or would observation status fit better?
- Continued stay: Is there enough documentation to support another hospital day?
- Procedure review: Does the record support why this service is needed now?
- Reimbursement link: Will the payer see the same medical necessity that the clinical team sees?
Why this role matters so much
Healthcare runs on both clinical care and documentation. If either side breaks down, patients can face delays and organizations can face denials, appeals, and unnecessary friction.
Practical rule: In UR, good care still needs good documentation. If the chart doesn't show it, the reviewer can't assume it.
That's why UR nurses often communicate with physicians, case managers, and other team members to clarify severity, timing, response to treatment, and the need for a certain level of care. The role protects patients from inappropriate or duplicate services, but it also supports access to necessary care by making sure the chart accurately reflects the clinical picture.
What utilization management is really trying to do
Major nursing organizations describe this work as part of utilization management, which exists to help ensure patients receive needed care while avoiding unnecessary or duplicate services. That balance can sound uncomfortable at first to nurses coming from the bedside.
But the role isn't about denying care for the sake of savings. It's about matching the right care to the right setting, at the right time, with documentation that supports the decision. When UR is done well, it supports both patient advocacy and responsible resource use.
A Day in the Life of a UR Nurse
Many nurses often find this aspect challenging. They understand the definition, but they still can't picture the actual workday.
That confusion is common. Most online content explains that UR nurses assess medical necessity, but rarely shows what the role looks like across prospective, concurrent, and retrospective review, or how the day splits between documentation and provider communication.
A typical day is less like bedside nursing and more like moving through a clinical decision queue. You log into the EHR, open payer portals, review assigned cases, compare chart details with criteria, send clarification requests, document determinations, and follow cases that need escalation or appeal support.
Here's a helpful video overview before we break down the workflow in plain language.
Prospective review before care happens
Prospective review happens before a service is delivered.
A common example is a planned surgery, imaging study, or specialty treatment that needs authorization. The UR nurse reviews the available record and checks whether the request meets payer rules and guideline criteria. If the documentation is complete and the case matches criteria, the request can move forward more smoothly.
If it doesn't, the problem often isn't the patient's condition. It's that the chart may be missing key details such as failed conservative treatment, symptom severity, prior interventions, or the reason a lower level of care won't work.
A prospective review day may include:
- Reviewing scheduled cases: Looking at upcoming procedures or admissions that need authorization support.
- Checking guideline fit: Comparing the request against MCG, InterQual, or payer-specific requirements.
- Requesting missing details: Messaging a provider office or care team for supporting documentation.
- Documenting the rationale: Recording why the case does or does not currently meet criteria.
Concurrent review during the hospital stay
This is the part many hospital-based UR nurses spend a lot of time doing. Concurrent review happens while the patient is actively receiving care.
You may review a new admission in the morning, then revisit another patient whose continued inpatient stay needs support. You're looking at vitals, labs, imaging, nursing notes, provider assessments, treatment response, and discharge barriers. Then you ask: does today's chart still support this level of care?
Sometimes the answer is yes. Sometimes the patient is improving and may no longer meet inpatient criteria, even though discharge planning is still in motion. That's where communication matters.
A strong concurrent reviewer doesn't just find problems. They spot what the chart needs before a denial happens.
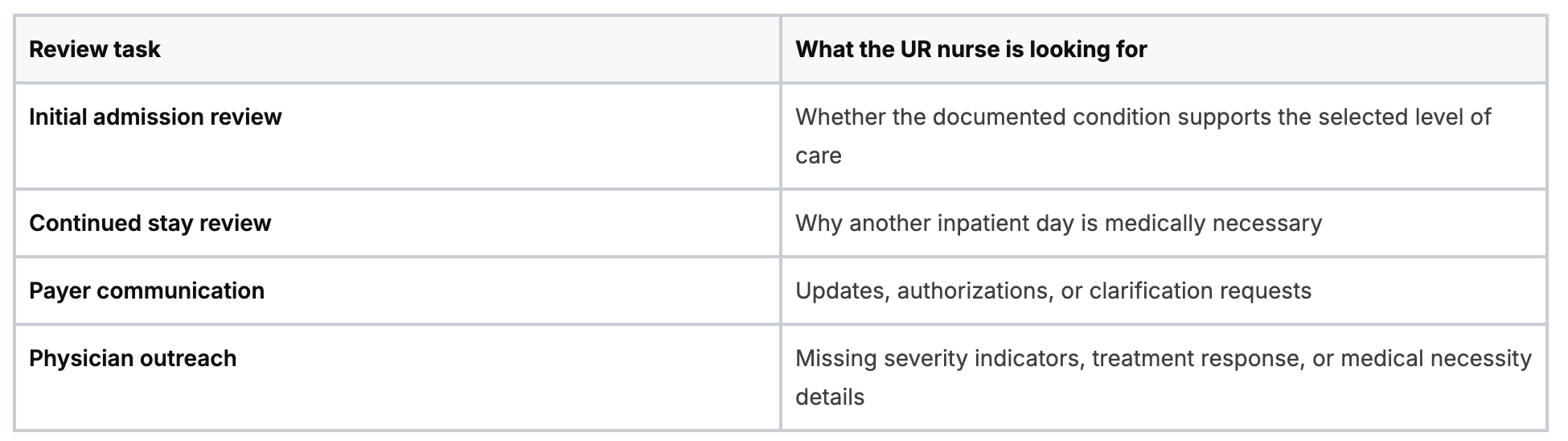
Common concurrent tasks include a mix of short and long reviews:
Retrospective review after care is complete
Retrospective review looks backward. The care already happened, and now the question is whether the record supports what was done.
This can be part of denial prevention, appeal preparation, internal audit work, or quality improvement. In these cases, the UR nurse studies the completed chart to see whether the care was appropriate and whether the documentation would stand up to payer review.
Retrospective work often teaches nurses a lot about patterns. You start to see where denials are likely to come from, which service lines struggle with documentation, and what details regularly get missed.
For many nurses, that's when the role clicks. It isn't just chart review. It's clinical pattern recognition applied in a different environment.
Key Skills and Credentials for Success
UR nursing rewards a different kind of stamina than bedside work. You may not be lifting patients or juggling a full assignment, but you are making repeated judgment calls from documentation, often with limited time and competing priorities.
That means the strongest UR nurses usually bring a blend of clinical experience, communication skill, and comfort with structured review tools.
Clinical experience still comes first
Most major-market job descriptions for utilization review roles require at least 2 to 3 years of prior clinical experience and often prefer BSN-level preparation plus quality or case-management credentials.
That makes sense. If you've worked med-surg, ICU, ED, step-down, rehab, or another acute-care setting, you already understand disease progression, escalation, treatment timing, and what “sick enough for this level of care” looks like in practice.
Without that foundation, UR can feel abstract. With it, the chart becomes easier to interpret.
The skills that matter most on the job
Some of the most important UR skills aren't flashy, but they matter every day:
- Clinical judgment: You need to tell the difference between a weak chart and a weak case. They aren't always the same.
- Documentation reading: UR nurses read closely. One overlooked progress note or missing treatment response can change the review.
- Written communication: Much of your work is documented in formal notes, payer systems, or internal review summaries.
- Provider communication: You need to ask concise, clinically sound questions without sounding adversarial.
- Workflow discipline: The work can involve queues, deadlines, follow-ups, and payer turnaround expectations.
- Tech comfort: You'll usually work across EHRs, payer portals, and review tools in the same shift.
Credentials and education
At minimum, most employers want an active RN license and relevant clinical experience. Many postings prefer a BSN, especially in larger systems or payer-facing roles. If you're still sorting out that educational path, this practical guide to RN vs BSN differences can help you understand how employers often view each route.
Some nurses also add case management, quality, or utilization-focused credentials later. These can strengthen your résumé, but they usually build on experience rather than replace it.
Where online education fits in
Continuing education matters in UR because payer rules, documentation expectations, and healthcare operations keep changing. Nurses moving into this specialty often need refreshers in documentation, compliance, care coordination, reimbursement concepts, and specialty-specific clinical topics.
Online learning works well for this kind of career development. It lets you study around shifts, revisit material, and focus on the exact gaps you need to close. For working nurses, that practical flexibility matters just as much as content quality.
If a course is accredited and relevant, the format matters less than whether it helps you apply the material on the job.
That's also why the old belief that only a narrow set of in-person classes count is fading. Healthcare education has moved forward. Accredited online CE and certification options are now a standard part of professional development for many nurses and employers. For a role like UR, where reading, judgment, and documentation are central, online learning is often a natural fit.
UR Nurse vs Case Manager Distinctions
These roles overlap enough to confuse almost everyone at first. Both may review charts. Both talk with providers. Both influence length of stay, discharge timing, and patient progression through the system.
But their primary lens is different.
The simplest way to separate them
A utilization review nurse focuses on whether the current service or level of care is medically necessary and supported by documentation.
A case manager focuses more broadly on the patient's overall care plan, coordination needs, discharge path, and barriers to safe transition.
Here's the clean comparison:
- UR nurse: does this admission, stay, or service meet criteria?
- Case manager: what does this patient need to move safely through care and out of the hospital?
How that looks in practice
Say a patient is hospitalized after a complex injury and may need transfer to another facility. The UR nurse reviews whether the inpatient stay still meets criteria today. The case manager works on discharge planning, placement, family communication, and post-acute logistics.
That distinction becomes even clearer in transport planning. If a patient needs transfer over a long distance, the clinical and logistical choices around air transport can involve different care coordination decisions.
Where the roles meet
They still work closely together.
- UR may flag status concerns: For example, whether inpatient criteria are still met.
- Case management may address discharge barriers: Such as placement delays or service availability.
- Both may communicate with physicians: But for different reasons.
- Both affect hospital flow: One through criteria review, the other through coordination.
In some organizations, one nurse may handle parts of both jobs. In others, the roles are tightly separated. If you're deciding between them, ask yourself what kind of work energizes you more. If you prefer analysis, payer criteria, and documentation logic, UR may fit better. If you prefer care coordination, patient-family problem-solving, and discharge planning, case management may feel more natural.
Job Outlook Salary and Work Settings
Utilization review has grown as healthcare organizations put more attention on cost control, payer rules, and evidence-based review. That trend has created steady interest in nurses who can connect clinical care with reimbursement logic.
One career guide projects 12% job growth from 2018 to 2028 for utilization review nurses, and the Bureau of Labor Statistics reported a median annual wage of $77,600 for registered nurses in 2021, which UR-focused sources suggest these roles often exceed because of their specialized demands.
Where UR nurses work
This specialty isn't limited to hospitals. UR nurses are found in several settings, and the day-to-day work changes depending on the employer.
- Hospitals and health systems: Reviewing admissions, continued stays, and status decisions.
- Health insurers: Evaluating authorization requests and coverage determinations.
- Managed care organizations: Applying payer criteria across broad populations.
- Independent review firms and vendors: Handling outsourced review work, audits, or appeals support.
Some roles are fully onsite. Others are hybrid or remote, especially when the work is heavily based in chart review, payer communication, and electronic workflow management.
Why the work setting matters
A hospital-based UR nurse often works close to bedside teams, case managers, and physician advisors. A payer-side UR nurse may spend more time applying plan criteria and less time interacting directly with unit staff. Vendor and independent review roles can be more process-driven and may involve high-volume review queues.
If salary is part of your comparison process, broad RN compensation benchmarks can help provide context. This 2026 registered nurse salary guide is a useful starting point for looking at the wider market before you narrow down specialty roles like UR.
The role is changing with policy and automation
UR nursing isn't static. Recent policy and workflow changes are pushing the work toward faster, more digital review processes.
In January 2024, CMS finalized a Medicare Advantage rule that speeds up prior authorization decisions, requires clearer denial explanations, and expands electronic prior authorization requirements over time. Alongside that shift, the CAQH 2024 Index reported continued administrative savings from automation in healthcare transactions, including prior authorization. In practical terms, that means UR nurses increasingly need to be comfortable with electronic workflows, standardized documentation, and tighter turnaround expectations.
The future of UR looks less like paper chasing and more like high-speed clinical review inside digital systems.
Advancing Your Career with Modern Education
If utilization review sounds like the kind of nursing work you'd enjoy, the path usually starts with the experience you already have. Acute-care practice gives you the clinical instincts. Then you build on that foundation with stronger documentation knowledge, familiarity with payer logic, and continuing education that keeps your skills current.
Many nurses still hear outdated advice. Some people continue to act like only in-person training from a small set of organizations counts. That view doesn't match how healthcare education works now. Accredited online CE and certification formats are widely used because they're practical, accessible, and well suited to working clinicians.
Why online learning fits a UR career path
UR work is built around reading, judgment, documentation, and application. Online education supports those same habits. You can move at your own pace, review complex material more than once, and fit coursework around your schedule instead of rearranging your life around a classroom date.
If you're comparing options for license renewal, skill-building, or role preparation, this guide to nurse continuing education is a useful place to start.
What to look for in your next step
Choose education that is:
- Accredited: So it meets professional and employer expectations
- Relevant: Focused on clinical review, documentation, or the specialty you want to move into
- Flexible: Built for nurses who are already working
- Practical: Easy to apply on the job, not just easy to finish
A utilization review nurse helps connect patient care, medical necessity, and system accountability. If you like clinical reasoning, careful chart review, and work that shapes decisions behind the scenes, it can be a strong next move.
If you're ready to build that next step with a flexible, accredited format, ProMed Certifications offers online certifications and continuing education designed for busy healthcare professionals. Their platform makes it easier to complete CE, maintain required credentials, and learn on your own schedule without sacrificing quality or credibility.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)