How to Avoid Fatigue: When Should Team Roles Alternate?
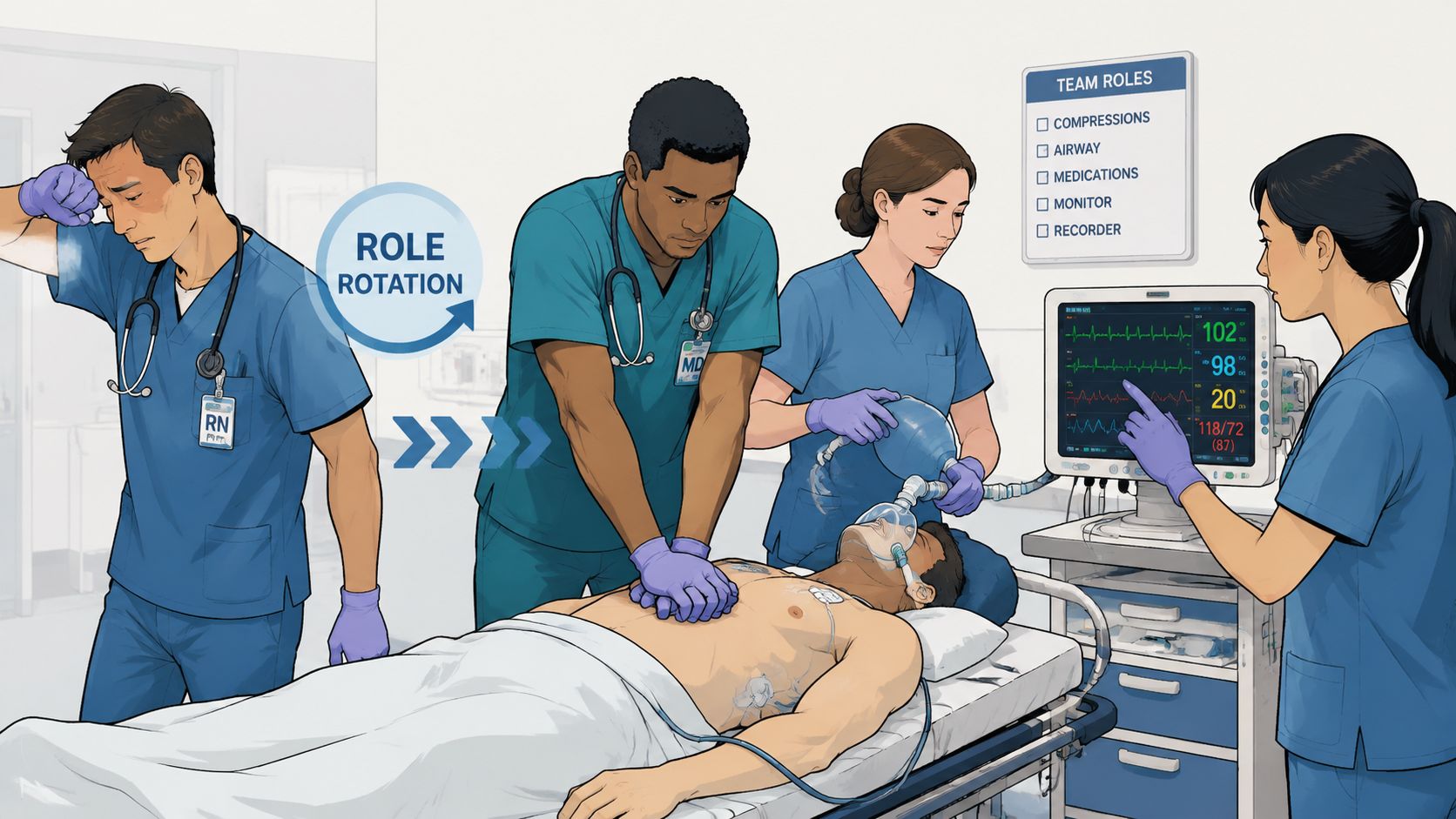
If you've ever been deep into a long code, you already know the moment. The room is still moving, alarms are still sounding, meds are still being called out, but the team has started to slow in ways nobody wants to admit. Compression depth gets questionable. The airway clinician asks for the same item twice. The recorder stops repeating times out loud. Nobody is panicking, but performance is no longer sharp.
That's the core question behind to avoid fatigue when should team roles alternate. It isn't just about following a memorized CPR rule. It's about protecting performance before physical strain, mental overload, and decision fatigue begin to affect care.
In high-stakes medicine, fatigue rarely announces itself dramatically. It shows up in smaller failures first. A delayed response. A missed cue. A handoff that takes too long. Good teams don't wait for obvious collapse. They rotate roles early, deliberately, and with a plan.
Why We Need to Talk About Team Fatigue
A prolonged resuscitation can feel deceptively controlled at first. Early on, adrenaline carries the room. People move fast. The compressor is strong. The team leader is thinking ahead. The airway clinician is calm and organized. Then the case stretches on, and the cost of staying in one role too long starts to show.

What makes team fatigue dangerous is that it affects both physical performance and clinical judgment. In a code, that means more than sore shoulders. It can mean slower rhythm recognition, weaker communication, and a growing risk of fixation. One person keeps doing the same thing because changing course takes more mental effort than they have left.
Fatigue hurts before anyone says they're tired
In practice, fatigue becomes visible long before someone asks for relief. The compressor leans more with the back than the hips. The medication nurse hesitates on a verbal order they would usually process instantly. The leader stops scanning the whole room and starts staring at the monitor.
That's why role alternation needs to be treated as a patient safety tool, not a courtesy. In broader fatigue management, one evidence-based principle is to alternate roles to support recovery, because extended shifts of 12 hours or more are more fatiguing than shifts of 8 hours or less as reduced recovery time increases sleep debt across consecutive shifts.
Clinical reality: Teams rarely fail all at once. They drift off target a little at a time.
The same principle shows up outside acute care too. If you're interested in the broader physiology and day-to-day burden of fatigue. Fatigue changes cognition, coordination, and stamina long before total exhaustion.
Burnout and acute fatigue often overlap
A clinician coming into a shift already depleted will fatigue faster during a long event. That's one reason operational resilience matters just as much as bedside skill. Chronic strain, understaffing, and repeated high-intensity assignments all raise the chance that your team reaches its limit sooner than expected. Proactive staffing habits and recovery culture matter, and so does addressing the bigger issue of preventing nurse burnout.
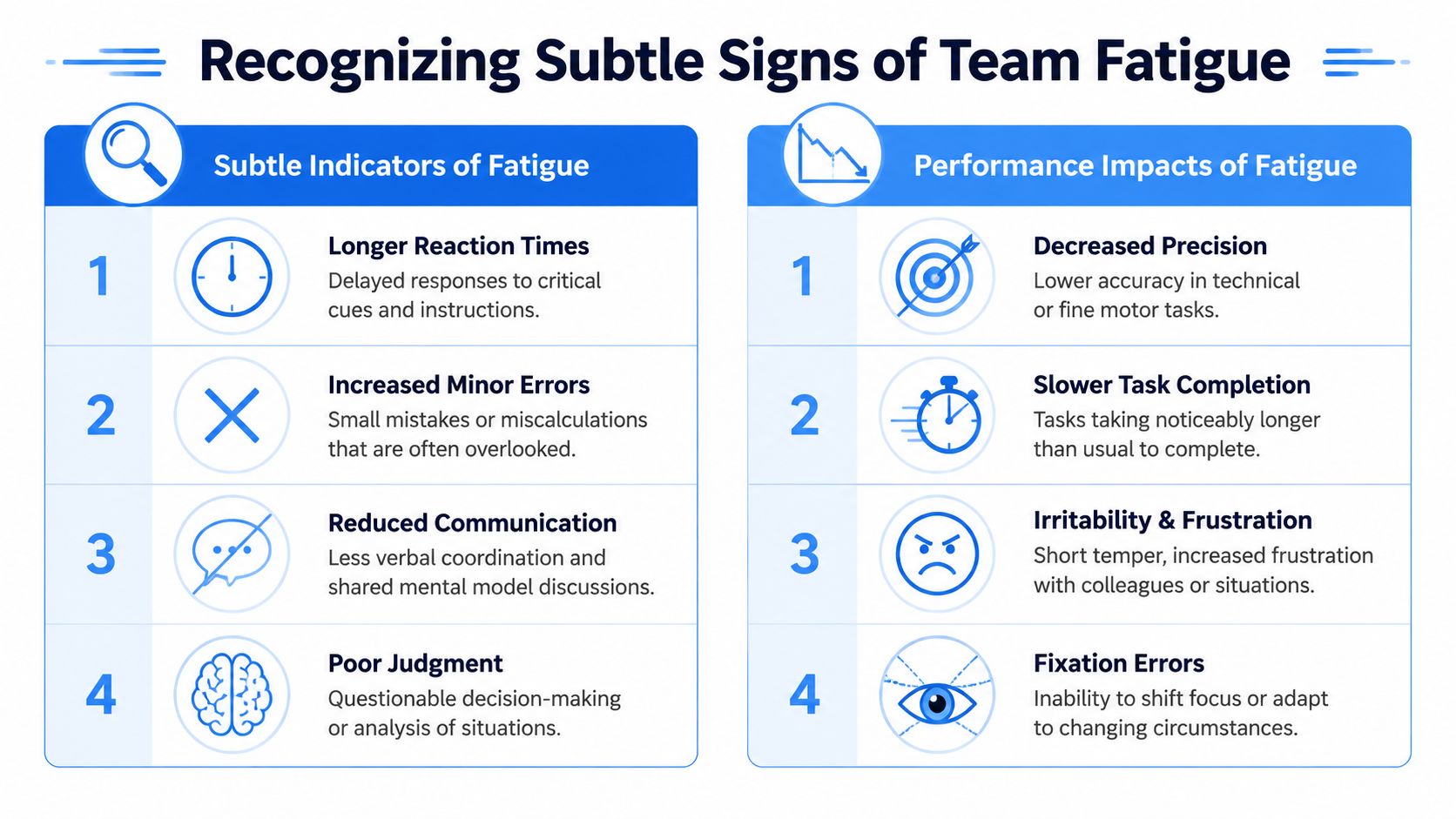
Recognizing the Subtle Signs of Fatigue in Your Team
Most fatigued clinicians don't look dramatically exhausted. They look slightly off. That's why team leaders need a working checklist in their head at all times, much like monitoring a patient. You're not waiting for arrest. You're looking for early deterioration.
What the team member feels
Some of the earliest signs are subjective. If your culture punishes people for admitting fatigue, you'll miss them.
- Shortened patience: The clinician becomes curt, defensive, or unusually frustrated over routine prompts.
- Narrowing attention: They stop tracking the whole scene and focus only on the task directly in front of them.
- Self-reported strain: If someone says they're fading, believe them the first time.
- Loss of confidence: Orders that would normally be simple start getting repeated or second-guessed.
What the team leader can see
Other signs are more objective and usually appear in performance before anyone names fatigue out loud.
- Compression quality slips: Depth becomes shallow, recoil gets incomplete, or body mechanics look inefficient.
- Response time lengthens: Requests have to be repeated. Equipment arrives late. Rhythm checks take longer to organize.
- Minor errors increase: Labels get missed, timing gets muddled, and routine steps suddenly require extra prompting.
- Fixation shows up: One clinician keeps pursuing the same line of thought even when the patient or scene has changed.
A practical way to think about it is this. Fatigue has vital signs. You can't always measure them with a monitor, but you can see them in behavior.
Watch the task, not just the person. A tired clinician may still look composed while their performance is already degrading.
Why context matters
Not all fatigue comes from the code itself. A clinician at the end of an overnight shift is different from a clinician fresh into days. That matters because extended work periods create more fatigue burden than shorter ones. The practical principle from the fatigue literature is straightforward. Longer stretches of work reduce recovery and increase sleep debt, especially across consecutive demands, which is why smart teams don't treat all providers as equally fresh when assigning roles.
Use a simple mental comparison during any prolonged event:
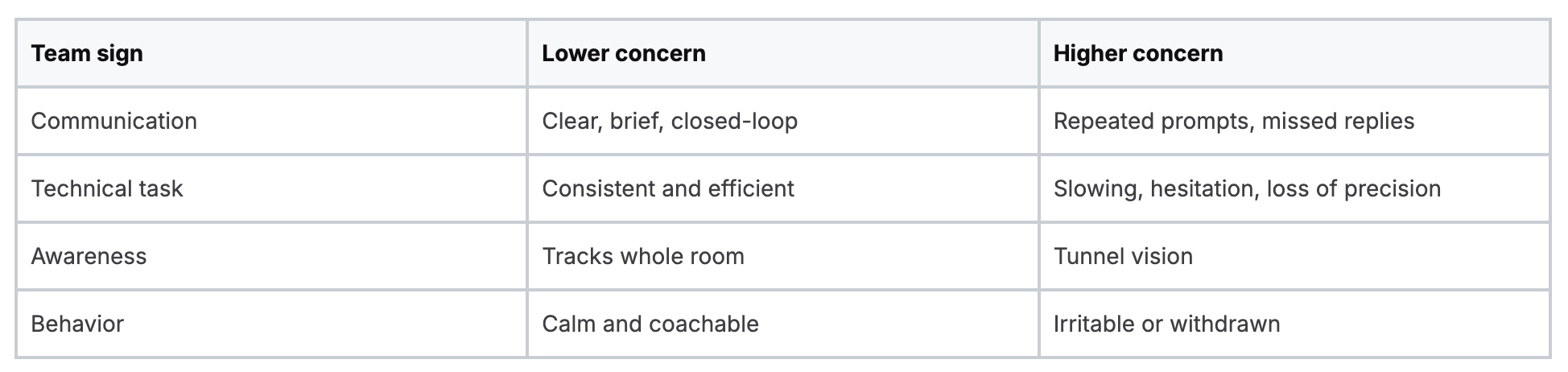
When you spot the higher-concern pattern, don't wait for a dramatic failure. Rotate early.
The CPR Compressor Swap Beyond the Two-Minute Mark
Everyone learns the standard rule. During CPR, compressors should switch about every 2 minutes or after about 5 cycles, and the switch should happen with an interruption of under 10 seconds, with earlier rotation if fatigue is visible.
That baseline matters. It gives teams structure when stress is high.

The mistake is treating 2 minutes like a target you must endure rather than a limit you shouldn't casually exceed. In real resuscitations, some clinicians need relief sooner. The patient does not benefit because the team hit a memorized interval while compression quality was already dropping.
When to switch before the clock says so
A strong team leader watches for quality-based triggers. If any of these show up, an early handoff is usually the safer move:
- Visible physical strain: Shoulder shaking, rising posture, compromised position, heavy breathing.
- Shallowing compressions: You can see the force fading even before anyone says it.
- Rhythm inconsistency: The cadence drifts or pauses creep in.
- Self-identified fatigue: The compressor says they're tiring. That is enough.
- Device or monitor concern: If your feedback tools suggest declining quality, act on that information.
If your team wants a refresher on what good compressions should look and feel like, chest compression depth and rate basics are worth reviewing with new staff and during mock codes.
How to keep the swap clean
The best compressor switch is almost boring. The next person is already in position. The team leader counts it down. The transition occurs during a natural pause, usually a rhythm check, and compressions resume immediately.
Don't admire endurance during CPR. Protect quality.
This is where training matters. Teams need to practice the physical choreography of switching, not just the concept. If people wait until a real arrest to figure out where to kneel, how to move around lines, or when to announce the handoff, pauses will lengthen.
A quick skills review can help cement that rhythm:
Rotating Roles for the Entire Clinical Team
The compressor isn't the only person who gets tired. That's the blind spot in most discussions about role alternation. Resuscitation teams include a broader set of functions, including team leader, airway, AED or monitor, IV or IO or medications, and timer or recorder. Fatigue in any one of those positions can affect the whole code.
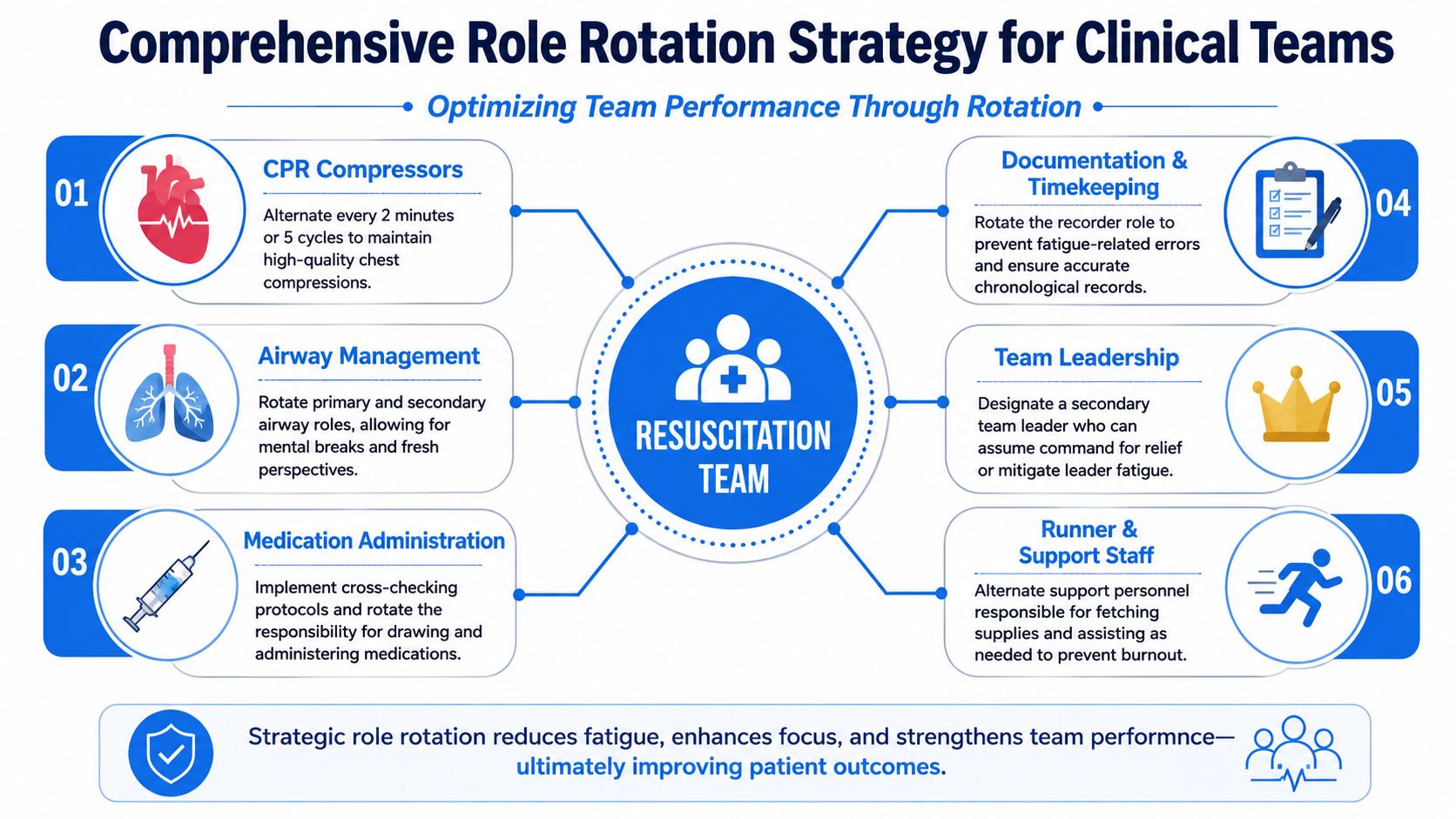
Cognitive roles fatigue differently
Physical fatigue is easier to spot. Cognitive fatigue is quieter and often more dangerous.
The airway clinician may start missing the bigger picture because all attention is locked onto the tube, mask seal, waveform, or suction. The medication clinician can become overloaded by repeated drug cycles, verbal orders, and calculations. The recorder may stop catching sequence errors because the running timeline has become mentally slippery.
That's why role rotation should be viewed as a whole-team strategy, not a compressor-only rule. If you need a clean model for who should be doing what during organized resuscitation, this summary of resuscitation triangle roles is a helpful starting point.
Practical triggers by role
Different jobs call for different thresholds.
- Airway role: Rotate when the clinician develops tunnel vision, repeated difficulty coordinating with compressions, or visible overload during a difficult airway sequence.
- Medication role: Consider a handoff when repeated rounds create confusion, dose confirmation slows down, or cross-checking starts to feel strained.
- Recorder or timer: Switch when verbal tracking gets delayed, time stamps lag, or the person stops anticipating key cycle points.
- Team leader: Relief may be appropriate when the leader is no longer scanning the room, isn't integrating input well, or has become so task-focused that command presence is slipping.
Understaffed teams need a different mindset
In a small ED, transport unit, or rural crew, you may not have spare hands. That doesn't mean rotation is impossible. It means rotation becomes more selective and more intentional.
A two-person or thinly staffed team can still use short cognitive resets, quick task trading during natural pauses, and preplanned secondary ownership. One person may remain primary in a role while another temporarily assumes verification, documentation support, or equipment setup to reduce overload.
The right question isn't "Can we rotate everyone?" It's "Which role is most likely to fail first if we don't?"
That reframes decision-making. In some cases, the airway role needs relief before the compressor. In others, the recorder is the weak link because the timeline is becoming unreliable. Good teams don't rotate symmetrically. They rotate where risk is rising.
Executing Smooth Handoffs and Planning for Contingencies
Knowing when to rotate is only half the work. The handoff itself has to be quick, clear, and structured. A sloppy transition can create the very error you were trying to prevent.
In safety-critical settings, task rotation works best as a proactive fatigue-control step, not as a last-minute rescue move. Guidance on worker fatigue prevention also notes that high-risk tasks may require breaks every 1 to 2 hours, with fatigue control built into operations before performance drops, especially during late-night or extended work periods, according to OSHA fatigue prevention guidance.
Use closed-loop language
When a clinician is nearing their limit, vague communication is dangerous. "I'm getting tired" may be heard and ignored. "Need help over here" may not identify who should respond.
Use direct handoff language instead.
- State the problem clearly
- "My compressions are getting shallow. I need a swap at the next pause."
- "I'm losing track of medication timing. I need another clinician to take meds."
- Assign the replacement
- "Alex, take compressions on my count."
- "Jordan, take over recording now."
- Confirm the transfer
- "I'm ready."
- "You have compressions."
- "I have compressions."
- Resume and reorient
- The outgoing clinician should either rest, move to a lower-load task, or support the incoming person briefly if needed.
- Primary and backup roles: Name who takes over if the first clinician fades.
- Expected fatigue points: Identify the tasks most likely to strain people physically or mentally.
- Micro-break opportunities: Even a brief step back, hydration pause, or cognitive reset can help when staffing is tight.
- Escalation plan: Decide when to call for added personnel rather than stretching the current team further.
- Role clarity: Who owns what in a code, and who backs them up.
- Early fatigue recognition: Spotting decline before errors become obvious.
- Closed-loop handoffs: Brief, direct communication under stress.
- Adaptation in low-resource settings: What changes when staffing is thin.
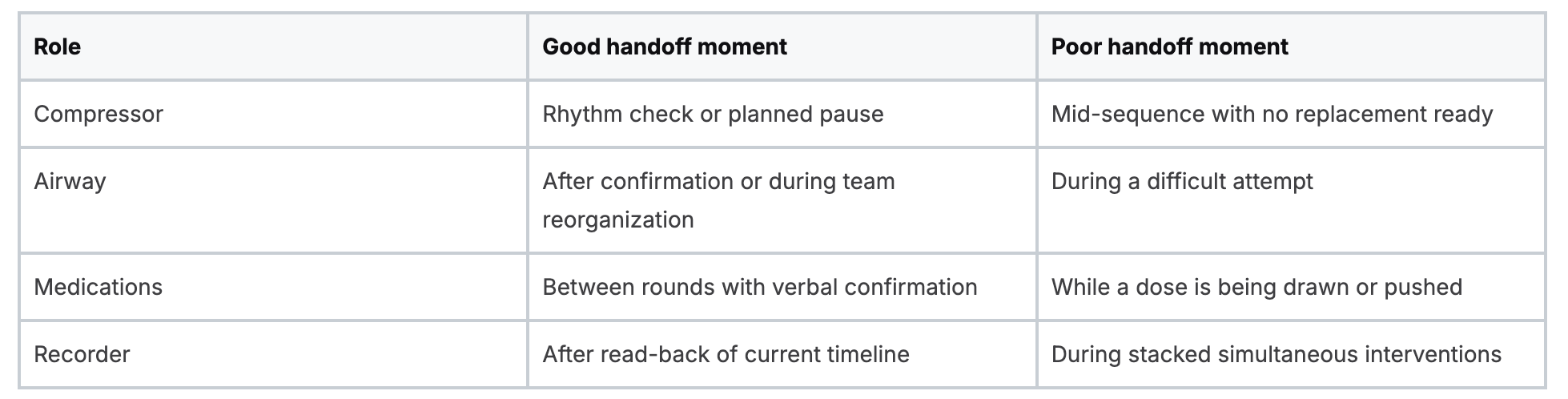
Handoffs work best during natural pauses
Not every role change should happen in the middle of a critical step. Aim for clean transition points:
Plan for the shift, not just the moment
Role alternation starts before the code starts. Teams should identify likely relief points early, especially during overnight work, long transports, or complex procedures.
A practical pre-brief can include:
In thin staffing models, this matters even more. You may not be able to give full relief, but you can still prevent overload by redistributing the highest-risk task before it breaks down.
Building a Fatigue-Resistant Team with Modern Training
A fatigue-resistant team doesn't improvise all of this under pressure. It trains for it. People need repetition in recognizing subtle fatigue, speaking up early, swapping roles cleanly, and working within staffing limits without losing structure.
That's one reason modern online education matters so much. Clinicians need access to frequent refreshers, scenario review, and skills reinforcement that fits real schedules. The old idea that only in-person classes from legacy organizations are valid is outdated. In practice, accredited online CE and certification pathways are widely used, highly practical, and increasingly accepted across healthcare settings.
Why online training fits this skill set well
Fatigue management isn't just memorization. It's judgment, timing, and communication. Online learning works well here because clinicians can revisit scenarios, pause, repeat, and study when they're able to focus. That flexibility matters for nurses, physicians, EMS professionals, and hospital teams trying to maintain competency around unpredictable schedules.
What I've seen repeatedly is simple. Teams get better at role alternation when training is accessible enough to revisit often. A single classroom day doesn't build durable performance by itself. Ongoing review does.
What strong training should reinforce
Look for education that helps clinicians practice:
Online CE and certification formats support all of that without forcing clinicians to chase limited classroom dates or assume that one brand's in-person card is the only acceptable option. Healthcare education is moving toward broader acceptance of flexible, accredited online training because it meets clinicians where they are and supports consistent review.
If you want a flexible way to strengthen resuscitation judgment, role clarity, and certification readiness, ProMed Certifications offers online ACLS, BLS, PALS, CPR, neonatal resuscitation, CE, and CME options built for busy healthcare professionals. You can train at your own pace, review material as often as needed, and keep your skills current without putting your schedule on hold.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)