Quality Improvement in Healthcare a Practical Guide
You're probably here because you've seen the same problem more than once.
A patient waits too long for discharge instructions. A handoff misses one critical detail. A checklist exists, but nobody uses it the same way. You do your part well, yet the system keeps producing the same avoidable friction. That's where quality improvement in healthcare becomes more than a management phrase. It becomes a practical skill set for people who are tired of watching good clinicians work inside flawed processes.
Done well, quality improvement helps you move from frustration to action. It gives teams a way to test changes, measure whether care is getting better, and build habits that last. It also builds your career. Clinicians, educators, and healthcare leaders who understand QI can lead safer workflows, stronger teams, and more reliable patient care.
Why Quality Improvement Matters Now More Than Ever
You've likely had a shift where everything felt one step harder than it should have been. Maybe the patient was ready to go home, but the discharge process stalled. Maybe a follow-up task fell between two roles, and everyone discovered the gap too late. These aren't always failures of effort. Often, they're failures of design.
That matters because the stakes in healthcare are high. The World Health Organization estimates that in low- and middle-income countries, 5.7 to 8.4 million deaths each year are attributed to poor-quality care, and in high-income countries, 1 in 10 patients is harmed while receiving hospital care, according to the WHO fact sheet on quality health services.

The problem is often the process
Most healthcare professionals enter the field to help people, not to redesign workflows. Still, many of the problems that frustrate staff and harm patients are process problems. The same delay, omission, or communication breakdown can happen again and again unless a team studies it and changes the system.
That's why quality improvement in healthcare isn't just paperwork. It's a method for making care safer, more reliable, and easier to deliver under real-world pressure.
Poor outcomes don't always mean people don't care. Often, they mean the system isn't helping people succeed consistently.
Technology is part of that effort, but only when it solves a real operational need. If you're seeing how digital tools can support better coordination and care delivery, this look at how medical practices are improving with technology is a useful companion.
QI turns concern into action
Quality improvement gives teams a structured response to recurring problems. Instead of saying, “We need to do better,” QI asks more useful questions:
- What exactly is going wrong
- How often is it happening
- What change are we testing
- How will we know if it helped
Those questions sound simple. In practice, they change everything. They shift the culture from reacting to incidents toward building systems that prevent them.
What Is Quality Improvement in Healthcare
Quality improvement in healthcare is the structured, ongoing work of making care better. Better can mean safer care, smoother workflows, stronger patient experience, fewer missed steps, or more reliable outcomes. The key is that QI is deliberate. Teams identify a problem, test a change, measure the result, and adjust.
Consider it similar to refining a recipe in a busy kitchen. If the meal comes out differently every time, you don't just tell the staff to “be more careful.” You standardize ingredients, sequence, timing, and checks so the result becomes repeatable.
QI is different from quality assurance
People often mix up quality improvement and quality assurance. They're related, but they aren't the same.

Quality assurance tends to look backward. It checks whether a requirement was met. Quality improvement looks forward. It asks how the work can be redesigned so good performance happens more consistently.
Why QI became data-driven
A major turning point came in 1924, when Walter Shewhart developed statistical process control, introducing the idea of using data over time to distinguish normal variation from a true process change.
That shift matters because healthcare teams can't rely only on before-and-after snapshots. A process might look better one week and worse the next. Shewhart's approach helped healthcare move from anecdote toward measurement over time.
Practical rule: If you don't know whether a change is producing a real signal over time, you don't yet know whether you improved the system.
The three outcomes most teams are chasing
Most QI work supports three connected aims:
- Safer care. Fewer missed steps, fewer preventable harms, and more reliable high-risk processes.
- Better outcomes. Care that achieves the intended clinical goal more consistently.
- Stronger efficiency. Less rework, fewer delays, and smoother handoffs so clinicians can focus on patients.
These aims overlap. A clearer triage process can improve safety and speed. Better discharge communication can support outcomes and reduce confusion. In strong QI work, the patient benefit and the workflow benefit usually rise together.
Exploring Core QI Frameworks and Models
No single framework solves every problem. The right one depends on what you're trying to fix. Some methods help teams test small changes quickly. Others help them map waste, reduce variation, or assess quality from a broader systems view.
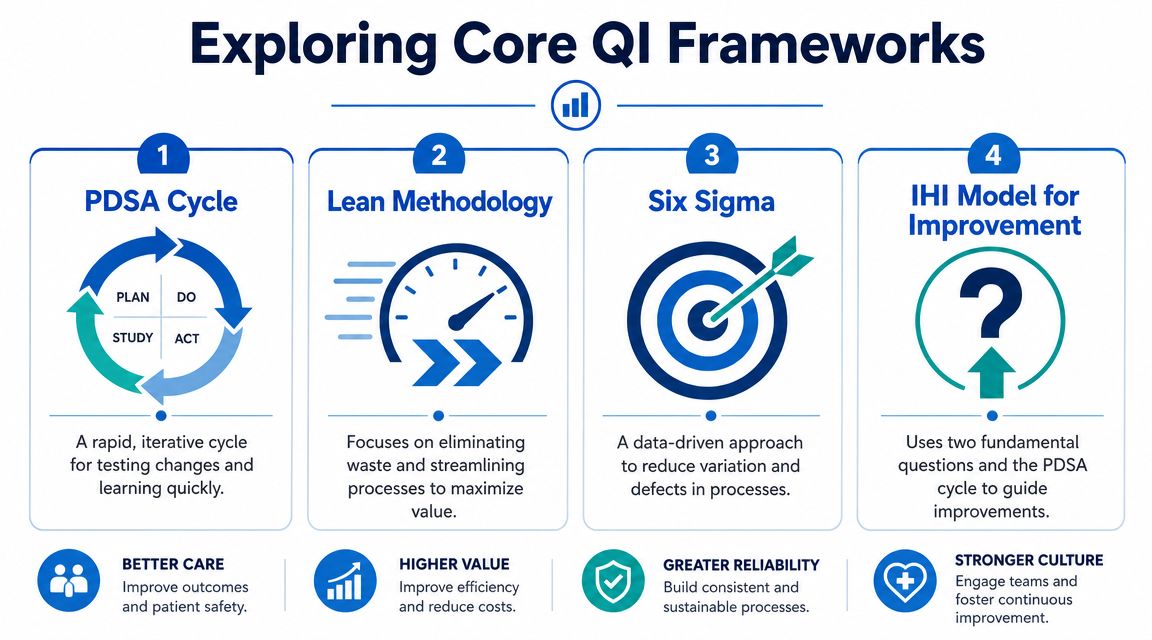
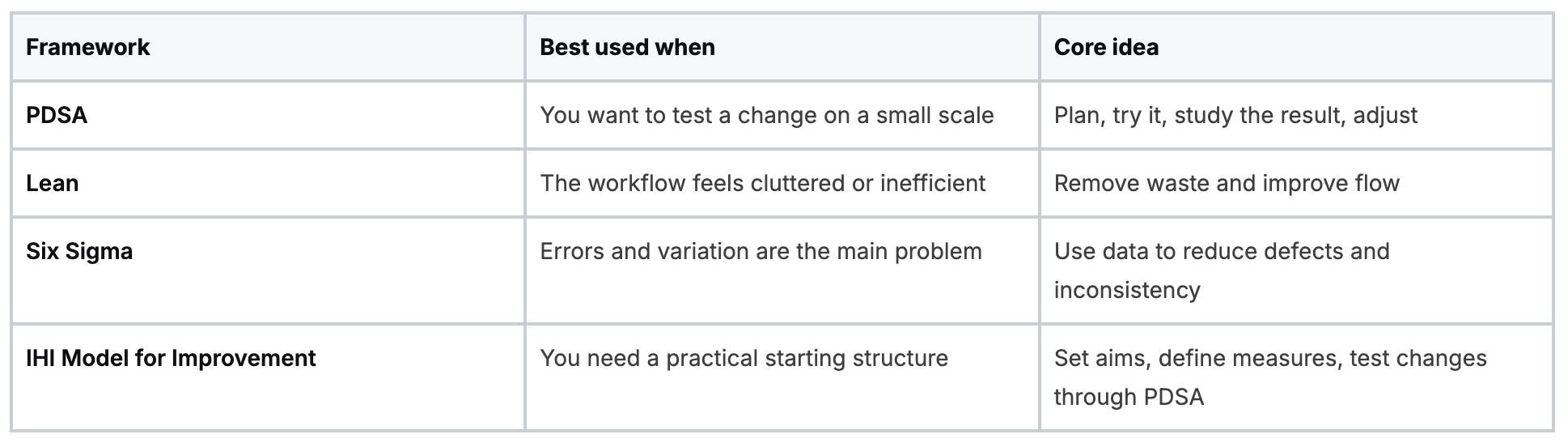
A side-by-side look at common models
PDSA works well for real clinical settings
Plan-Do-Study-Act is often the most approachable model for frontline teams. It doesn't require a huge launch. You identify a specific change, test it on a small scale, review what happened, and decide what to adapt.
That makes PDSA useful when teams are unsure whether a change will work in their setting. For example, if discharge teaching feels rushed, a team might test a revised handoff script with one clinician group before expanding it.
Lean focuses on waste you can feel every day
Lean is helpful when staff keep saying things like, “We do too many extra steps,” or “This process makes no sense.” It asks where time, motion, duplication, and bottlenecks are getting in the way of value.
In healthcare, waste doesn't just mean supplies. It can mean:
- Repeated documentation that adds no patient value
- Unclear handoffs that force staff to chase information
- Workflow delays that leave patients waiting without a clinical reason
Lean can be especially useful in outpatient flow, triage, room turnover, and discharge processes.
Six Sigma is stronger when precision matters most
Six Sigma is more data-heavy. It's built to reduce variation and defects. In healthcare, that can matter when a process must happen the same way every time, especially in areas where inconsistency creates risk.
This model tends to fit well when teams have enough data and a clearly defined process problem. If every clinician completes a task differently and those differences affect reliability, Six Sigma thinking can help.
A fast process isn't always a good process. A consistent process that protects patients is usually the better starting point.
The IHI model is practical for beginners and leaders
The IHI Model for Improvement is popular because it asks three straightforward questions:
- What are we trying to accomplish?
- How will we know a change is an improvement?
- What changes can we make that will result in improvement?
Then it uses PDSA cycles to test answers. That combination makes it useful for teams that want structure without getting buried in jargon.
If you're new to quality improvement in healthcare, this model often feels the most usable because it connects aims, measurement, and testing in one workflow.
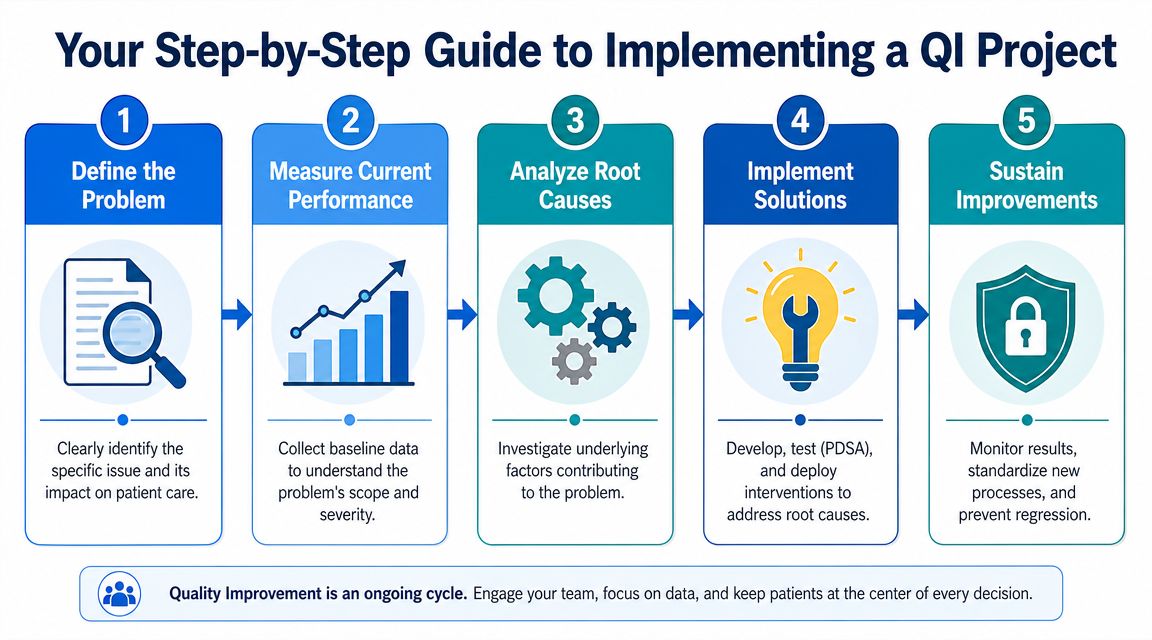
Your Step-by-Step Guide to Implementing a QI Project
A good QI project doesn't begin with a giant committee meeting. It starts with a problem that's specific enough to study and important enough to matter. “Communication needs improvement” is too broad. “Discharge instructions are incomplete on weekend shifts” is something a team can work with.
Start with a problem you can define
The first task is to describe the issue in plain language. Name where it happens, who is involved, and why it affects patient care. A narrow project usually works better than a vague, organization-wide ambition.
Then build a team with the people who touch the process. That often includes clinical staff, support staff, and someone who understands the workflow data.
Measure before you change anything
Effective quality improvement is a measurement system. AHRQ and CMS emphasize defining a baseline, tracking process measures tied to the intervention, and comparing pre-change and post-change performance, as outlined in the AHRQ guide to quality improvement approaches.
If you skip the baseline, you'll struggle to answer the most important question later. Did the change help, or did the process just fluctuate?
A simple roadmap often looks like this:
- Define the problem clearly. Keep it observable and tied to patient care.
- Measure current performance. Capture what's happening before you intervene.
- Look for root causes. Ask why the problem repeats.
- Test a change on a small scale. Don't roll out everything at once.
- Review the results. Decide whether to adopt, adapt, or stop.
- Standardize what works. Build the new process into daily practice.
Root cause analysis needs honesty
Many teams often get stuck when they identify the symptom, not the cause. If medication reconciliation is inconsistent, the issue may not be staff knowledge. It might be confusing ownership, poor timing in the workflow, or documentation fields that don't match the clinical sequence.
Useful questions include:
- Where does the process break down most often
- Who has to improvise to keep things moving
- What step depends on memory instead of a prompt or standard
- What happens on nights, weekends, or high-volume days
Test small, then spread carefully
The smartest QI teams don't launch everything to everyone at once. They test a change with one team, one shift, or one unit. That lowers risk and makes learning faster.
Start small enough that failure is informative, not disruptive.
After a successful test, write the new standard into the workflow. Update checklists, train staff, clarify ownership, and keep monitoring. Improvement that isn't sustained becomes a short-term project, not a system change.
Choosing the Right Metrics for QI Success
Many QI projects fail because they pick weak measures. The team works hard, rolls out a change, and ends up with data that can't answer whether care improved. Good metrics are less about collecting more numbers and more about choosing the right ones.
The three kinds of measures that matter
A practical QI measurement set usually includes three categories.
- Outcome measures track the result you care about. These are the patient-facing or system-level effects of the work.
- Process measures tell you whether the new steps are being performed as intended.
- Balancing measures help you spot unintended consequences somewhere else in the system.
If a team changes triage workflow, an outcome measure might reflect timeliness or safety, a process measure might examine use of the new triage method, and a balancing measure might check whether another part of the clinic became less efficient.
Why process measures are often overlooked
Teams usually care most about outcomes, and that makes sense. But outcomes can lag. Process measures tell you sooner whether the intervention is being used consistently enough to have a chance of working.
For example, a checklist can't improve care if staff don't complete it at the right point in the workflow. That's why process measurement is often the bridge between good intentions and reliable practice.
WHO recommends tools such as clinical registries, checklists, and validated triage tools to reduce failure points and improve data use for redesigning care, as described on the WHO clinical quality improvement page.
Run charts help you see change over time
A single monthly report can hide what's really happening. A run chart gives you a simple visual of data over time so you can see whether a process is shifting or just bouncing around.
That's especially helpful when teams get confused by short-term variation. One better week doesn't prove the intervention worked. One bad week doesn't prove it failed. Looking across time helps you avoid overreacting and underreacting.
The most useful metric is one your team can act on, not one that only looks impressive on a dashboard.
Common Pitfalls in Quality Improvement and How to Avoid Them
Most QI projects don't struggle because the team doesn't care. They struggle because the work is harder than it first appears. Clinical environments are busy, priorities compete, and a good idea can collapse if the process around it is weak.
Common reasons projects stall
Some problems show up again and again:
- The aim is too broad. If the goal is fuzzy, nobody knows what success looks like.
- The team skips baseline measurement. Then they can't prove whether anything improved.
- Frontline staff weren't included. The redesigned workflow doesn't match real work.
- The change adds burden. Staff stop using it because it slows them down.
- There's no sustainment plan. Once the initial attention fades, the old process returns.
Burnout also matters. Improvement work has to fit the reality of clinical labor. If your team is already stretched thin, this guide on dealing with burnout in the medical profession offers useful context for protecting staff while still making progress.
Average improvement can hide unequal outcomes
One of the most important QI mistakes is assuming that a better average means better care for everyone. A major challenge in quality improvement in healthcare is that disparities can persist or worsen if teams don't explicitly measure race, ethnicity, and language data and design interventions for underserved populations.
That means a project can look successful on paper while leaving some patients behind.
How to avoid that equity trap
A safer approach includes a few habits:
- Stratify results when possible. Don't rely only on the average.
- Review access barriers. Ask whether the intervention works equally well across different patient groups.
- Watch incentives carefully. Avoid designs that make high-risk patients seem like a problem to avoid.
- Include community and patient perspectives when the project affects underserved populations.
QI should make systems fairer, not just faster.
Building Your Skills with Modern Training Options
Quality improvement is a professional skill, not just an organizational initiative. Clinicians who understand measurement, workflow design, and implementation can lead projects, contribute more effectively to committees, and make stronger decisions at the bedside and system level.
What strong QI learners need
You don't need to become a full-time quality director to benefit from QI training. Most professionals need a practical mix of abilities:
- Reading process problems clearly
- Choosing measures that fit the intervention
- Testing changes without creating chaos
- Communicating findings to leaders and peers
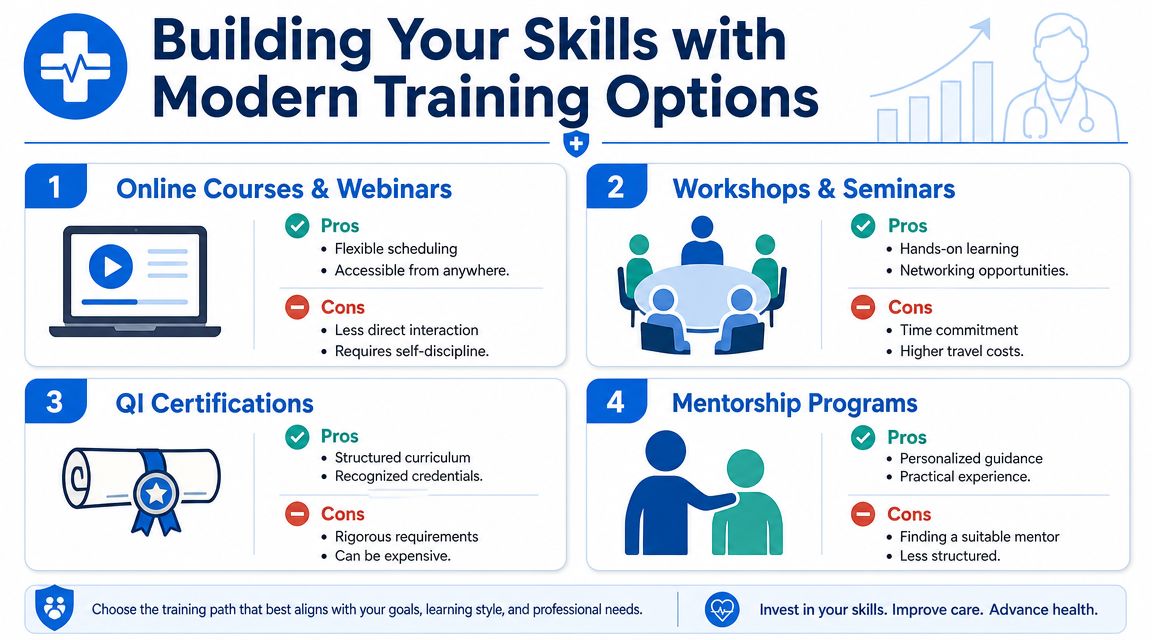
Online learning is a valid path for modern clinicians
There's still a stubborn belief in some settings that meaningful healthcare education only happens in person. That view is outdated. For continuing education and certification, online learning is widely used because it fits clinical schedules, reduces travel friction, and lets professionals review material at a practical pace.
That matters for QI training because the subject is applied. You need space to think, revisit examples, and connect tools to your own workflow. Online formats often support that better than a rushed classroom day.
A range of accredited options now support healthcare professionals through online education, including continuing medical education online. For clinicians building formal quality skills, one available option is ProMed Certifications, which offers online medical certification courses, and ProMed Academy also offers a CPHQ exam preparatory course tied to healthcare quality competencies.
The bigger point is simple. AHA and American Red Cross in-person classes are not the only valid route for professional development. Accredited online education is accepted across many healthcare settings and matches how busy professionals learn today.
If you're ready to turn quality improvement knowledge into a practical career asset, ProMed Certifications offers online certification and continuing education options built for working healthcare professionals. You can complete coursework on your schedule, access accredited content, and build skills that support both patient care and professional growth.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)