

Nursing Care Plan for Pneumonia

You have report in hand, meds to reconcile, and a new admission rolling up from the ED with fever, cough, fatigue, and worsening shortness of breath. The diagnosis says pneumonia. The chart says a lot. Your patient says even more.
This is the moment when a nursing care plan for pneumonia stops being a school assignment and becomes a working clinical tool. You are not filling boxes. You are deciding what matters first, what can wait, what needs a call, and what should already be in motion before the provider arrives on the floor.
New nurses often get stuck here for one reason. They try to write the whole plan at once. Experienced nurses do the opposite. They assess first, identify the immediate threats, set realistic goals, and document in a way that helps the next nurse take over without guessing.
Your Guide to Crafting an Effective Pneumonia Care Plan
Start with the patient, not the template.
An older adult arrives from the ED with a productive cough, low oxygen saturation on room air, coarse breath sounds, and visible fatigue from the work of breathing. Before you think about wording a diagnosis, you are already noticing priorities. Air movement. Oxygenation. Secretions. Tolerance for activity. Hydration. Safety.

A strong nursing care plan for pneumonia does three jobs at once:
- Guides your next actions: It helps you decide what to do now, what to reassess soon, and what to escalate.
- Keeps the team aligned: Respiratory therapy, providers, aides, and the next shift can all see the same clinical picture.
- Shows your clinical reasoning: Your interventions are tied to actual findings, not copied from a generic list.
Think of the care plan like a bedside map. The diagnosis names the problem, but the map shows the route. If your patient starts to desaturate, becomes more lethargic, or cannot clear secretions, that map helps you act quickly because you already identified the likely trouble spots.
Preceptor tip: If your care plan does not change what you are watching for or what you are doing at the bedside, it is too vague.
The best plans are dynamic. They tighten when the patient worsens and simplify as the patient stabilizes. That is what makes them useful in real practice.
Laying the Foundation Your Essential Assessment
When nurses say, “the patient doesn’t look good,” they are usually integrating dozens of assessment cues at once. Your job is to slow that instinct down and turn it into data you can act on.
Pneumonia remains a leading cause of global morbidity and mortality, and care plans commonly aim for oxygen saturation above 92% within 24 to 48 hours with respiratory assessments often performed every 4 hours, including monitoring for airway patency and gas exchange.
Start with what tells you the patient is stable or not
A respiratory rate, oxygen saturation, temperature, heart rate, and blood pressure are not isolated numbers. Together, they tell a story.
A patient with tachypnea, fever, and low oxygen saturation may be compensating hard. They can still be talking to you and still be getting into trouble. Pneumonia patients often look “okay” right up until they tire out.
Focus first on bedside signs of respiratory strain:
- Work of breathing: Look for nasal flaring, use of accessory muscles, inability to speak comfortably, or visible fatigue.
- Oxygenation: Compare current SpO2 with oxygen delivery. Room air and 2 L nasal cannula are not the same clinical picture.
- Mental status: Restlessness, confusion, or sudden sleepiness can be early signs that oxygenation is worsening.
Build a respiratory assessment that means something
Do not settle for “lungs diminished” unless that is all you hear. Auscultation should help you decide what problem is most urgent.
Crackles can point you toward fluid and alveolar involvement. Rhonchi suggest secretions that may move with coughing. Diminished sounds can mean poor air movement, shallow breathing, or more serious compromise.
You also want to assess the cough itself. Is it weak or effective? Is the patient bringing anything up? Thick sputum that stays in the airway changes your care priorities immediately.
A focused note often includes:
- Breath sounds: Crackles, rhonchi, wheezes, diminished areas, symmetry
- Cough quality: Strong, weak, painful, productive, dry
- Sputum findings: Color, thickness, amount, odor if present
- Chest discomfort: Especially with coughing or deep breathing
- Tolerance to position changes: Some patients desaturate or become markedly dyspneic with minimal movement
If you want a structured refresher on organizing this bedside work, this review of head-to-toe assessments is useful for tightening your routine.
Subjective data matters more than new nurses think
Patients often tell you the change before the monitor does.
“Breathing feels harder today.”
“I can’t clear this junk.”
“I’m too tired to walk to the bathroom.”
“My chest hurts when I cough.”
Those statements shape your care plan because they connect symptoms to function. Pneumonia is not only about gas exchange. It affects sleep, mobility, appetite, hydration, and willingness to participate in treatment.
In older adults, family members may give you the clue that matters most. A daughter who says, “She is usually sharp, and today she is confused,” may be identifying decline before the chart catches up. If pneumonia is part of a larger caregiving picture, resources on recognizing when a parent needs help can help families understand when a change at home has become a safety issue.
Key takeaway: Assessment is not data collection for its own sake. Every finding should help you answer one bedside question. Is this patient oxygenating, ventilating, clearing secretions, and tolerating the effort of breathing?
Do not forget the practical findings
Pneumonia care becomes harder when basic needs are missed.
Check hydration status. Fever and rapid breathing can dry a patient out and make secretions harder to mobilize. Look at intake, mucous membranes, urine output trends, and whether the patient can drink without exhaustion.
Assess mobility carefully. A patient who can ambulate at baseline may now need help just to sit at the bedside. That matters for fall risk, secretion clearance, and discharge planning.
A good assessment gives you the raw material for the whole plan. Without it, the nursing care plan for pneumonia becomes generic. With it, your interventions become precise.
Prioritizing Nursing Diagnoses What Needs Your Attention Now
A pneumonia patient may qualify for several nursing diagnoses at once. The trap is treating them as equal. They are not.
Maslow helps here, but so does basic bedside urgency. If oxygenation is threatened, that diagnosis moves to the top. If secretions are blocking air movement, airway clearance rises quickly. Pain, fever, fatigue, and hydration all matter, but they come after the problems most likely to worsen gas exchange.
In severe cases such as ventilator-associated pneumonia, mortality can reach 25% to 50%, and structured care plans emphasize immediate airway management with pulse oximetry monitoring every 2 to 4 hours according to NurseTogether’s pneumonia nursing diagnosis care plan guide.
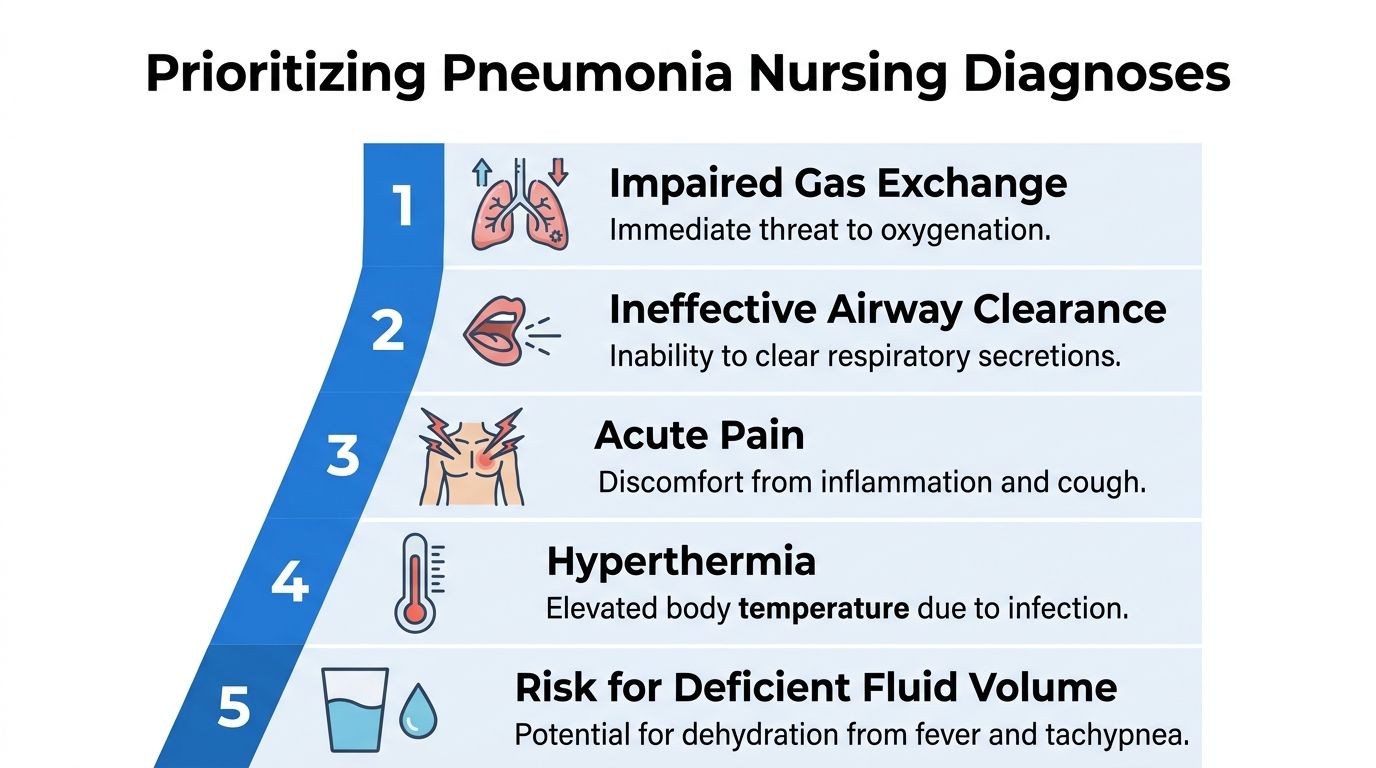
First priority impaired gas exchange
This diagnosis belongs near the top when your assessment shows low oxygen saturation, abnormal ABGs if available, dyspnea, cyanosis, worsening fatigue, or signs of increased work of breathing.
The reasoning is simple. Inflamed or fluid-filled alveoli are not exchanging oxygen well. That is an immediate physiologic threat.
You are not choosing this diagnosis because pneumonia affects the lungs in general. You are choosing it because your patient is showing evidence of impaired oxygen transfer.
A precise statement might sound like this:
Impaired Gas Exchange related to alveolar inflammation and fluid accumulation as evidenced by low oxygen saturation, dyspnea, and abnormal breath sounds.
Second priority ineffective airway clearance
Some pneumonia patients are oxygenating poorly because they cannot move secretions. Others are on the edge of worsening because the cough is weak, painful, or exhausted.
This diagnosis moves up when you hear rhonchi, observe a weak or ineffective cough, note thick sputum, or see the patient avoid deep breathing because it hurts.
Ask yourself one bedside question. Can this patient clear what is in the airway without help?
If the answer is no, your plan should reflect that immediately.
Problems that matter next
Once oxygenation and airway clearance are addressed, several other diagnoses commonly come into focus.

These are not “lower importance” because they are minor. They are less urgent than airway and oxygenation in the first round of prioritization.
Tie each diagnosis to actual findings
New nurses often write broad diagnoses that could fit half the unit. The chart gets stronger when your wording clearly reflects your patient.
Compare these two examples:
- Too vague: Ineffective Airway Clearance related to pneumonia
- Better: Ineffective Airway Clearance related to retained secretions as evidenced by rhonchi, productive cough, and difficulty expectorating thick sputum
The second version tells the next nurse what problem exists and what evidence supports it.
Preceptor tip: If your “as evidenced by” section contains findings you did not personally assess or verify in the chart, stop and tighten it up.
Use urgency, not habit, to rank them
You will not always rank diagnoses the same way. A patient with mild hypoxia but severe exhaustion and very poor secretion clearance may need airway-focused interventions first. Another patient may have acceptable breath sounds but a dropping oxygen saturation that points you toward gas exchange.
That is why a real-world nursing care plan for pneumonia is dynamic. It starts with structure, but it depends on clinical judgment.
A quick bedside ranking tool can help:
- What can harm the patient fastest? Usually oxygenation or airway.
- What is driving the problem? Secretions, inflammation, fatigue, pain, dehydration.
- What is limiting treatment participation? Pain, weakness, confusion, fear.
- What could become a complication if ignored? Falls, worsening fatigue, poor intake, delayed mobilization.
When you prioritize this way, your care plan starts sounding less like school paper language and more like clinical thinking.
Crafting SMART Goals and Evidence-Based Interventions

You have identified the priority problem. Now you need to decide what improvement should look like by the end of your shift and what nursing actions are most likely to get the patient there.
New nurses often lose time at this stage. They write a broad goal, add a familiar list of interventions, and only later realize the plan does not help with reassessment or documentation. A stronger pneumonia care plan works like a bedside map. It points to the next safe action, the next reassessment, and the next charted response.
Write goals the bedside nurse can measure
A SMART goal should answer five practical questions. What should improve? How will you measure it? By when? Under what support or treatment? How will the next nurse know whether it happened?
For pneumonia, avoid goals that sound good but cannot be checked. “Patient will breathe better” is too loose to guide care. “Patient will maintain ordered oxygen saturation target on prescribed oxygen by end of shift, with decreased dyspnea at rest” gives you something you can reassess and document.
Here is the difference in practice:
- Too broad: Patient will improve respiratory status.
- Usable at the bedside: Patient will maintain ordered SpO2 goal on prescribed oxygen during this shift and show reduced work of breathing after repositioning, oxygen therapy, and coached breathing.
That second goal saves time later because it already tells you what to look for.
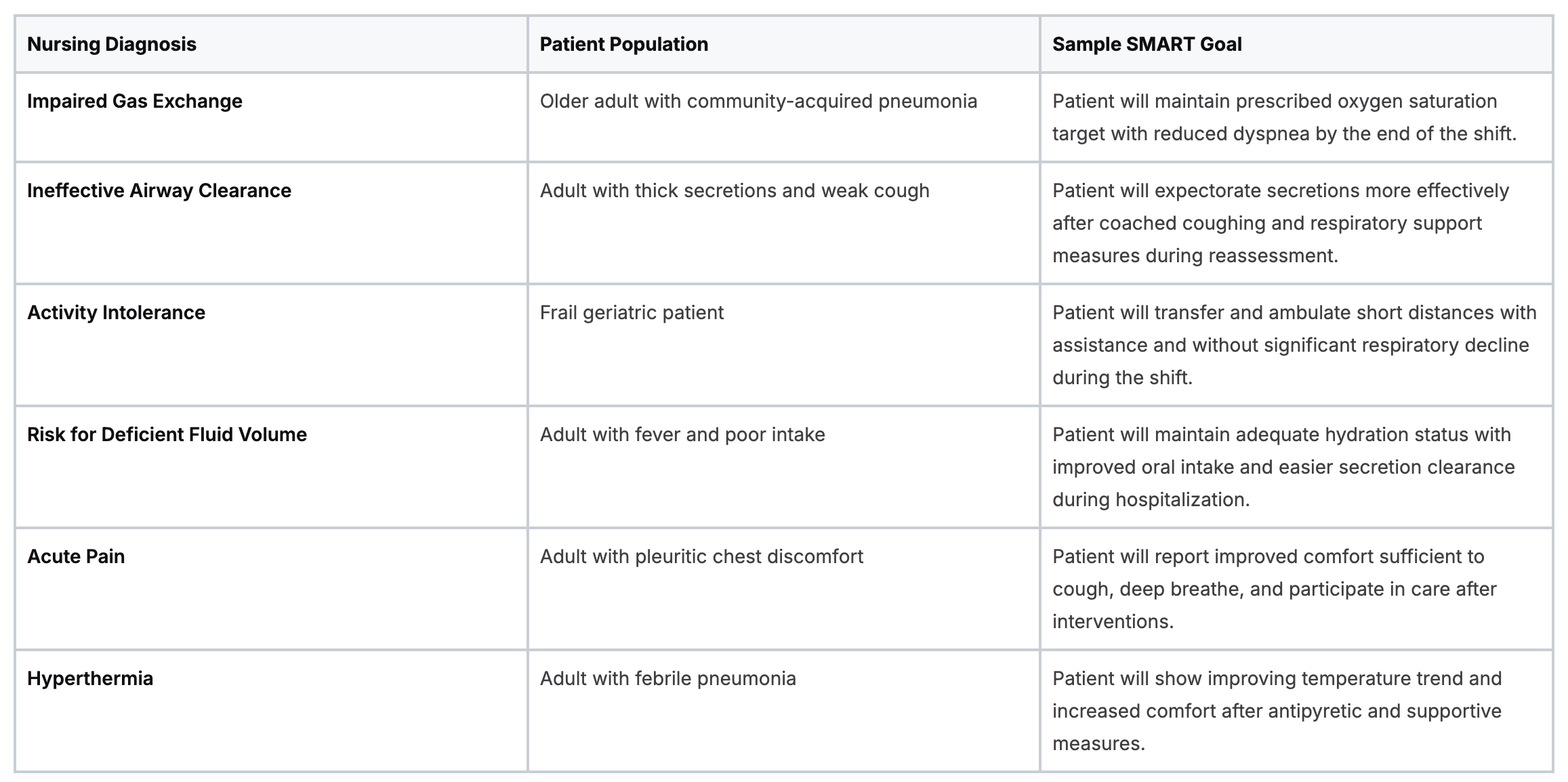
Examples you can adapt:
- Impaired Gas Exchange: Patient will maintain the ordered oxygen saturation target on prescribed oxygen within this shift.
- Ineffective Airway Clearance: Patient will produce sputum more effectively and demonstrate a stronger cough by reassessment.
- Activity Intolerance: Patient will transfer or ambulate a short distance with assistance and without marked increase in respiratory distress during this shift.
- Risk for Deficient Fluid Volume: Patient will maintain adequate intake and show easier secretion clearance during hospitalization.
A quick table you can adapt in practice
Match interventions to the specific problem in front of you
A diagnosis label helps organize your thinking. It does not replace your thinking.
Two patients can both carry “Ineffective Airway Clearance,” but one mainly needs pain control before coughing and the other needs upright positioning, fluids, and frequent coaching because fatigue is limiting secretion clearance. Your interventions should reflect the barrier.
For secretion clearance, choose actions that help the patient move mucus, not just receive instructions.
- Coach deep breathing and coughing: Stay specific. Tell the patient when to inhale, when to hold, and when to cough.
- Use incentive spirometry as ordered: Explain the purpose, set a realistic schedule, and reassess effort and technique.
- Support hydration if not contraindicated: Thinner secretions are easier to mobilize.
- Reposition and mobilize: Sitting upright and getting to the chair often improves lung expansion more than repeated reminders from the bedside.
For gas exchange, focus on oxygen delivery and the mechanics of breathing.
- Adjust oxygen per orders and policy: Reassess after each change.
- Use positioning intentionally: Semi-Fowler’s or higher may reduce work of breathing and improve ventilation.
- Monitor the patient, not just the monitor: Respiratory rate, accessory muscle use, sentence length, skin color, and anxiety often show change before the number settles.
For activity intolerance, pace care instead of stacking demands.
- Cluster care thoughtfully: Give the patient recovery time between effort-heavy tasks.
- Coordinate pain relief, respiratory treatments, and mobility: The order matters. A patient who is more comfortable and less short of breath is more likely to cough, sit up, and walk.
- Set a small mobility target: “Chair for meals” or “walk to doorway with assist” is easier to achieve and evaluate than “increase activity.”
Rationales should sound like clinical judgment
A useful rationale answers one question. Why does this action fit this patient right now?
Good rationales are short and specific:
- Upright positioning promotes lung expansion and may improve oxygenation.
- Hydration support can help loosen secretions and make cough more productive.
- Pain control before coughing exercises increases participation in deep breathing and secretion clearance.
- Clustered care reduces oxygen demand and fatigue in a patient already working hard to breathe.
Weak rationales create extra charting without adding meaning. “To help patient feel better” is not wrong, but it is too general to show your reasoning.
Teach while you intervene
Pneumonia care often feels repetitive to the patient. Cough again. Sit up again. Use the spirometer again. Drink again. Walk again.
A brief explanation improves cooperation. The spirometer helps reopen air sacs. Sitting up gives the lungs more room to expand. Fluids help loosen secretions. Coughing clears what antibiotics cannot mechanically remove. That kind of teaching turns the care plan into something the patient can participate in, not something being done around them.
Family teaching matters too, especially near discharge. If the patient will need help managing antibiotics, inhalers, or follow-up medications at home, these medication management tips for caregivers can support your discharge teaching.
If the patient worsens suddenly, this review of what to do if someone has a respiratory arrest is a useful companion resource for emergency response thinking.
A visual review can help connect these actions to bedside care.
Key takeaway: The strongest pneumonia interventions are tied to a clear bedside goal, matched to the patient’s actual barrier to improvement, and written clearly enough that reassessment and charting feel straightforward instead of rushed.
Closing the Loop Evaluation and Smart Documentation
It is 1500, and you are reassessing the patient you admitted this morning with pneumonia. They are on oxygen, they sat in the chair once, and you already taught coughing and deep breathing. The question now is not whether the tasks were completed. The question is whether the patient is breathing better because of them.
That shift in thinking is what turns ADPIE from a school assignment into real clinical practice. In pneumonia care, evaluation is your feedback check. It tells you whether to continue the plan, revise it, or escalate concern before the patient slips backward.
Evaluate the patient’s response in a way that guides your next decision
A completed intervention is not the outcome. Your reassessment needs to answer a bedside question: what changed after your care?
For a patient with pneumonia, that usually means checking for patterns in oxygenation, work of breathing, breath sounds, cough strength, sputum clearance, pain, fatigue, hydration, and tolerance for activity. You are comparing the patient’s current state to the goal you wrote earlier.
A simple way to organize your thinking is to ask:
- What was the problem?
- What did I do for it?
- How did the patient respond?
- What needs to happen next?
That sequence works like closing a circuit. If the response matches the goal, keep going. If the response is partial, adjust the plan. If the patient worsens, act quickly and notify the provider.
Here is what meaningful evaluation can sound like in practice:
- Oxygenation improving: Patient maintained target oxygen saturation after repositioning, oxygen therapy, and coached breathing.
- Airway clearance improving: Cough is stronger and more productive after hydration, upright positioning, and guided coughing.
- Activity tolerance still limited: Patient became tachypneic and dyspneic with transfer to chair. Activity goal needs to be scaled back and rebuilt gradually.
- Condition needs escalation: Fatigue, respiratory effort, or oxygenation worsened despite interventions. Provider and respiratory therapy notified.
Documentation should show your clinical reasoning, not just your task list
New nurses often worry that good charting means writing more. Usually, it means writing more clearly.
Your note should help another nurse see the patient’s story without hunting through the chart. A strong entry shows three things: what you assessed, what you did, and what happened after. That format is fast, defensible, and useful during handoff.
A practical charting pattern looks like this:
- Assessment finding: “Coarse crackles at bases, productive cough, dyspnea with exertion.”
- Intervention: “Repositioned upright, coached deep breathing and coughing, encouraged oral fluids, administered oxygen per order.”
- Response: “Patient expectorated sputum, states breathing is easier, oxygen saturation improved on reassessment.”
That note is short, but it carries clinical value. It shows why you intervened, what action you took, and whether the plan is working.
Know when the plan needs revision
A pneumonia care plan should change as the patient changes. Static plans miss early deterioration and waste time on interventions that are not helping.
Revisit the plan when:
- The patient is not meeting the stated goal
- The priority problem has changed
- The intervention does not fit the patient’s strength, tolerance, or condition
- A new issue appears, such as confusion, poor intake, worsening fatigue, or rising oxygen needs
Picture a patient who is too weak to complete coughing exercises on schedule. The original intervention may have been reasonable at the start of the shift. After reassessment, the better plan may be to coordinate coughing after pain medication, involve respiratory therapy, shorten activity demands, and document the barrier clearly so the next nurse does not repeat an unrealistic expectation.
Preceptor tip: If you keep charting the same intervention and the patient keeps showing the same poor response, revise the care plan.
Smart charting saves time for the whole team
Clear documentation does more than protect your license. It saves the next nurse from starting over.
A good note tells the oncoming nurse what the patient’s lungs are doing now, which interventions helped, what the patient could not tolerate, and what concerns still need follow-up. That makes handoff safer and more efficient.

This is the part of care planning that often saves the most time. Good evaluation sharpens your next intervention. Good documentation sharpens the next nurse’s assessment. That is how a pneumonia care plan becomes a working clinical tool instead of a form completed once and forgotten.
Advance Your Practice with Modern Continuing Education
Pneumonia care looks straightforward on paper until you are balancing oxygenation, secretion clearance, fatigue, mobility, family teaching, and charting in real time. That skill set improves with repetition, but it also improves with focused continuing education.
Nurses and other clinicians no longer have to rely only on classroom-based formats to stay current. Online education is a valid, effective option for CE and certifications, and many healthcare professionals now choose it because it fits real schedules better. The old assumption that only in-person AHA or American Red Cross classes count is outdated. High-quality accredited online options are widely used across healthcare settings.
That shift makes sense. Online learning gives clinicians flexibility, faster access, and the ability to review material at their own pace. For busy nurses, that matters. It means you can sharpen clinical judgment without waiting for a classroom seat or rearranging a full workweek.
If you want to keep building practical bedside skills, this guide to nurse continuing education is a helpful place to start.
The most valuable education does not just help you pass a renewal. It improves your next shift. In pneumonia care, that means recognizing deterioration earlier, writing tighter goals, choosing more precise interventions, and documenting in a way that supports continuity of care.
If you are ready to strengthen your clinical knowledge with flexible, accredited online training, ProMed Certifications offers future-focused CE and certification options designed for busy healthcare professionals. You can complete courses on your schedule, maintain compliance, and build skills that carry directly into patient care.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)
.png)