

LMA vs Endotracheal Tube: A Clinician's Guide

You’re often making the airway choice before the room feels settled. The monitor is on. The team is moving. Someone asks whether you want the LMA opened or the ETT prepared. That moment isn’t really about memorizing a pros-and-cons list. It’s about judgment.
The best clinicians don’t treat lma vs endotracheal tube as a trivia question. They treat it as a decision algorithm. You weigh aspiration risk, ventilation needs, procedure length, patient anatomy, and your own ability to place the device quickly and correctly. When you understand the why behind each option, the choice gets faster and safer.
The Critical Choice in Airway Management
Airway management can look simple on paper. In practice, it rarely feels simple. A patient who is stable at induction can become harder to ventilate than expected. A routine case can turn into a difficult airway. A short procedure can suddenly require tighter control of ventilation.
That’s why the LMA and the ETT matter so much. They solve different problems.
- The laryngeal mask airway or LMA sits above the vocal cords and creates a seal around the laryngeal inlet.
- The endotracheal tube or ETT passes through the vocal cords into the trachea and creates a more definitive airway.
Think of the difference like this. An LMA is often a well-fitted cover over the airway entrance. An ETT is a tube placed directly into the airway itself. Both can ventilate a patient. They just offer different levels of control, protection, and invasiveness.
What makes this a judgment call
You’re not picking the “better” device in the abstract. You’re picking the safer device for this patient, in this setting, with these risks.
A few questions usually drive the decision:
- Is aspiration a major concern
- Will the patient need high-pressure ventilation
- Is this a short elective procedure or a critical illness
- Do I need fast rescue ventilation right now
- What’s the likelihood of a difficult laryngoscopy
Airway skill isn’t just procedural. It’s the ability to match the device to the situation before the situation gets worse.
Competency also depends on staying current. Airway algorithms, rescue strategies, and monitoring standards keep evolving. For busy clinicians, that matters when choosing how to renew ACLS, PALS, BLS, or other certifications. Online education has become a practical way to maintain that readiness, and many healthcare employers now recognize accredited online training as a valid option. The old assumption that only in-person classes from a few major organizations count isn’t accurate anymore.
Understanding the Laryngeal Mask Airway
The LMA is a supraglottic airway. That means it sits above the glottis rather than passing through the vocal cords. Its cuff is designed to rest over the laryngeal inlet and create a seal that allows oxygenation and ventilation.
.png)
How the LMA works
A simple way to picture it is this. The LMA doesn’t enter the windpipe. It sits at the doorway and seals the entrance well enough to support ventilation in the right patient and procedure.
That design changes the insertion process. You’re generally not performing laryngoscopy to pass through the cords. In many routine uses, placement is faster and mechanically simpler than intubation. That’s one reason LMAs became so important in anesthesia and rescue airway management.
Clinically, the LMA is often useful when you need an airway that is less invasive but still more reliable than basic mask ventilation.
Why clinicians like it in the right case
The appeal of the LMA isn’t convenience alone. It’s the combination of speed, usability, and physiologic gentleness.
A meta-analysis found that one-time implantation success was substantially higher in the LMA group than in the endotracheal intubation group, with an OR of 0.20 and P=0.003, and heart rate variability was significantly lower with a mean difference of -13.76 and P<0.00001, which supports the idea that LMA placement can produce less physiologic stress during airway management.
That matters at the bedside. Less hemodynamic disturbance can be especially helpful when you want to avoid adding stress during induction or airway rescue.
For a practical placement walkthrough, this laryngeal mask airway placement guide is a useful refresher.
When it fits best
LMAs are commonly chosen for:
- Short elective procedures where a definitive tracheal tube isn’t necessary
- Rescue airways when ventilation is needed quickly
- Situations with difficult intubation where a supraglottic device can stabilize the patient first
Clinical mindset: An LMA is often at its best when you need a secure enough airway fast, but you don’t need the full protection of a tracheal tube.
A short demonstration helps make the device mechanics more intuitive:
Mastering the Endotracheal Tube
The ETT is the definitive airway standard because it goes where the LMA does not. It passes through the vocal cords into the trachea. That location gives you a more secure seal, better protection from aspiration, and tighter control over ventilation.
.png)
Why the ETT is considered definitive
When a cuffed ETT is placed correctly, you have direct access to the trachea. That changes what you can do for the patient.
You gain:
- Better aspiration protection
- More controlled positive-pressure ventilation
- Access for suctioning the lower airway
- A more dependable airway for longer or more complex cases
This is why the ETT remains the preferred choice in many high-risk settings, including patients with a full stomach, major trauma, prolonged surgery, severe respiratory failure, or situations where airway control has to be as complete as possible.
What makes it harder
ETT placement usually requires more technical skill. You’re aligning anatomy, visualizing the cords, advancing the tube, confirming position, and securing it. Even in experienced hands, it demands more than LMA placement.
That’s the trade-off. You get more control, but you pay for it with greater invasiveness and a steeper skill requirement.
A straightforward way to think about it is:
- You assess the airway and the patient’s risks
- You perform laryngoscopy and pass the tube through the cords
- You confirm placement with clinical assessment and capnography
- You secure the tube and manage ventilation
Capnography deserves special attention here. If you work in airway management, this guide to quantitative waveform capnography is worth reviewing because confirmation is not the place for guesswork.
The ETT is what you choose when airway protection and ventilatory control matter more than ease of placement.
Common scenarios where ETT leads
The ETT usually moves to the front when the patient needs a protected airway, not just a patent airway.
That includes:
- High aspiration risk
- Need for prolonged ventilation
- Poor pulmonary compliance or high airway pressures
- Critical illness with rapidly changing physiology
In other words, if the main question is “How do I control this airway completely,” the ETT usually answers it.
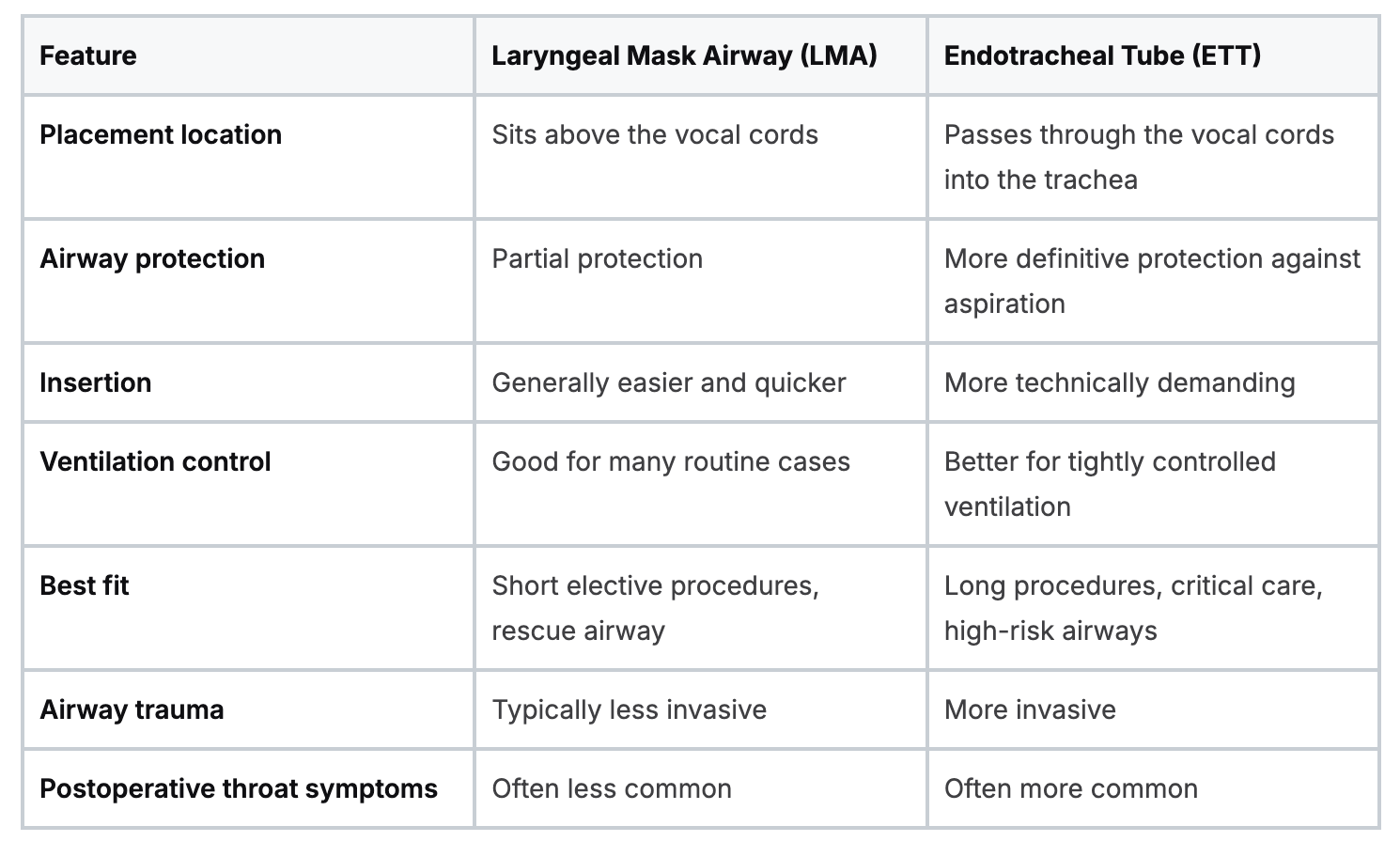
LMA vs ETT Key Differences at a Glance
The fastest way to compare lma vs endotracheal tube is by looking at the clinical problems each device solves. The decision gets clearer when you stop asking which one is best overall and start asking which one is best for aspiration protection, insertion speed, pressure control, and post-procedure comfort.

Speed and insertion stress
If speed matters, the LMA often has the edge. Comparative studies reported that LMA-Supreme insertion achieved an effective airway in 18.6 ± 5.1 seconds compared with 25.2 ± 8.3 seconds for ETT placement, with less hemodynamic disturbance and fewer sore throats.
Those same comparisons also noted systolic blood pressure rise under 15% with LMA versus 25% to 40% with ETT, and postoperative sore throat incidence under 10% with LMA versus 20% to 40% with ETT in the cited review.
That doesn’t make the LMA universally superior. It means the device may be more patient-friendly when the airway doesn’t require the full protection of an ETT.
Aspiration protection
This is the big dividing line.
An LMA can support ventilation very well, but it does not provide the same level of protection against gastric contents entering the lungs. The ETT does a better job here because it sits inside the trachea and seals it more definitively.
The central trade-off: The LMA is often easier on the patient and easier to place. The ETT protects the airway more completely.
Ventilation capability
Both devices can ventilate. The question is how much control you need.
If you expect changing compliance, prolonged ventilation, or the need for higher pressures, the ETT usually gives you more room to manage the patient. If ventilation demands are moderate and the case is appropriate, the LMA may be entirely suitable.
Skill requirement and workflow
There’s also a team factor. LMAs can be valuable when speed and simplicity improve workflow, especially in elective anesthesia or as a rescue device in difficult airway pathways. ETT placement requires more training, repetition, and confirmation discipline.
A simple mental model helps:
- Choose LMA when you want a fast, less invasive airway and the risk profile supports it.
- Choose ETT when you need protection, precision, and durable airway control.
- Reassess continuously because the right answer can change as the case changes.
Making the Call in Real-World Scenarios
A patient is oxygenating well in pre-op. Twenty minutes later, the same patient may need higher airway pressures, Trendelenburg positioning, or rescue ventilation after a failed intubation attempt. That is why airway choice is a thinking skill, not a memorized preference list.

The useful question is not, “Which device is better?” The useful question is, “What problem am I solving right now, and what is most likely to change next?” An LMA and an ETT are tools for different jobs. Good clinicians keep reassessing because the job can change quickly.
Scenario one in the operating room
A healthy patient is scheduled for a short elective procedure. They are appropriately fasted, aspiration risk appears low, and the case is expected to end without major shifts in ventilation needs.
In that setting, many anesthesia teams consider an LMA because it can support the case with less airway stimulation and a simpler workflow. The benefit is practical, not theoretical. If the procedure is brief and uncomplicated, the airway plan does not need to be heavier than the situation requires.
The key question is margin. If you expect the patient to remain easy to ventilate and easy to wake, an LMA may fit the case well. If new information appears, such as reflux history, full stomach concern, or unexpectedly poor ventilation, the decision changes with it.
Scenario two in laparoscopic surgery
Laparoscopic cases force you to think one step ahead. Pneumoperitoneum and positioning can change respiratory mechanics after the airway is already in place, so the initial choice has to account for what the abdomen and diaphragm may do later.
A randomized trial in laparoscopic surgery found comparable oxygen saturation and end-tidal CO2 between LMAs and ETTs, while respiratory mechanics differed between groups, as summarized in this randomized trial on respiratory mechanics with LMA and ETT. That does not make the LMA the default for every lap case. It means the decision should come from patient selection, expected airway pressures, positioning, aspiration risk, and the team’s backup plan.
This is a good example of why habit can mislead. “Laparoscopy equals ETT” is simple, but simplicity is not the same as judgment.
Scenario three in the emergency department or prehospital setting
You attempt intubation. The view is poor. Saturation is falling.
At that moment, the priority is oxygen delivery, not winning a difficult laryngoscopy attempt. A rescue supraglottic airway can restore ventilation fast, buy time, and let the team reset for the next move in the difficult airway plan. That is one reason clinicians should keep reviewing advanced airway options and best practices, not just the mechanics of placement but the decision points around rescue use.
Teams perform better in these high-stress moments when roles and triggers are standardized before the case ever starts. If your department is trying to reduce confusion during airway emergencies, a practical guide for consistent team procedures can help turn informal habits into repeatable workflow.
A practical decision algorithm
A simple way to organize the choice is to move through four questions.
- What can hurt this patient fastest?
If aspiration is the immediate concern, an ETT usually gives you the safer path. - What will ventilation probably require?
If you expect rising pressures, long duration, or changing lung mechanics, the ETT often provides more control. - What needs to happen in the next 30 seconds?
If oxygenation is failing and intubation is delayed, an LMA may be the fastest way to restore ventilation. - What is my exit plan?
Every airway choice should include a trigger for conversion, escalation, or calling for help if the situation shifts.
That is the practical skill clinicians need to practice. You are not choosing between two devices in the abstract. You are matching the device to the problem, then staying ready to change course when the problem changes.
Maintaining Competency with Modern Training
Airway management skill fades when it isn’t practiced. That’s true for both LMA placement and endotracheal intubation, and it’s also true for the decision-making around them. Clinicians need education that keeps pace with current practice, not just a checkbox course every renewal cycle.
There’s a training gap here. An analysis of healthcare education trends identified a significant lack of training that addresses practical considerations for airway device choice, which supports the need for more thorough educational programs, as discussed in this analysis of education gaps around airway device choice.
Why online learning fits modern airway education
This is one area where online education makes practical sense. Busy nurses, physicians, respiratory therapists, and compliance teams need access that fits real schedules. They also need current material they can revisit, not a single classroom session they’re expected to retain indefinitely.
The belief that only in-person classes from AHA or the American Red Cross are valid is outdated. Accredited online education is widely used, increasingly accepted, and well aligned with how clinicians maintain knowledge. For CE, CME, and many certification pathways, online learning can be just as effective while giving learners more flexibility and less disruption to work.
A focused review resource like this advanced airway options and best practices article works well because it supports spaced learning. You can return to key concepts, compare devices, and reinforce decision points when you need them.
Competency doesn’t come from where you sit during training. It comes from whether the training is accurate, current, and usable in patient care.
Your Airway Decision Framework
A useful airway framework has to work at 2 a.m., with alarms sounding and a patient who is changing in front of you. That is why the lma vs endotracheal tube decision should feel less like recalling a pros-and-cons chart and more like running a short clinical algorithm.
Start with the question that changes everything. Does this patient need airway protection from aspiration, or do they need the fastest path to oxygenation while you stabilize the situation? An ETT gives you a cuffed, tracheal airway when protection and tighter control matter most. An LMA sits above the glottis and can get oxygenation and ventilation started quickly when speed, simplicity, or rescue placement is the immediate priority.
From there, layer in the next questions. How much ventilatory control do you need? Will the procedure increase airway pressure demands? Is this a short elective case, a deteriorating emergency, or a bridge to something more definitive? Clinicians who make good airway choices do not ask, “Which device is better?” They ask, “What problem am I solving first?”
A simple way to remember the sequence is:
- Protect with an ETT when aspiration risk or definitive airway control leads the decision
- Rescue and ventilate with an LMA when rapid placement and oxygenation are the main goals
- Match the device to the setting by factoring in procedure type, duration, airway pressures, and patient anatomy
- Reassess early because the right first device may become the wrong device if the patient or procedure changes
This approach also explains why clinicians may choose different devices in similar-looking cases. Two patients can both need anesthesia, yet one has a full stomach and poor pulmonary reserve, while the other is fasting, stable, and scheduled for a brief low-risk procedure. The correct answer changes because the clinical priorities change.
That is the skill worth practicing.
Confidence in airway management comes from understanding the reason behind the choice, then being ready to change course when the situation demands it. If you’re ready to strengthen that judgment with flexible, accredited training, explore ProMed Certifications. Their online courses for ACLS, PALS, BLS, CPR, and more are built for busy healthcare professionals who want current, practical education without being limited to in-person-only options.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)
.png)