

Mental Health Crisis Intervention: Essential Skills

A patient on a general medical floor pulls off the pulse oximeter, accuses staff of trying to poison him, and starts pacing toward the door. He had surgery yesterday. No one called psychiatry because this didn't look like a psychiatric admission. Now the room is loud, the team is split on what to do, and every second feels longer than it is.
That moment is where mental health crisis intervention becomes a core clinical skill, not a specialty extra. Nurses, physicians, techs, paramedics, and allied staff all run into behavioral emergencies in places that weren't built for them. The job isn't to win an argument or force calm. The job is to create enough safety, structure, and clinical clarity to move the patient toward the right next step.
The First Five Minutes of a Mental Health Crisis
The first five minutes are about stabilizing the scene before you try to solve the story. Agitation, paranoia, suicidal statements, panic, intoxication, delirium, and psychosis can all look chaotic at the bedside. Your first response has to be simple enough to use under pressure.
Start with three questions:
- Is anyone in immediate danger right now
- Could this be a medical problem presenting as behavior
- Who needs to be in the room, and who needs to leave
A crowded doorway usually makes things worse. One calm lead communicator is better than five people talking over each other. Reduce the audience. Lower your voice. Ask a nearby staff member to secure obvious hazards and call for the level of support your facility uses for behavioral escalation.

What matters before words work
If the patient is post-op, elderly, hypoxic, withdrawing, septic, hypoglycemic, or newly confused, don't assume a primary psychiatric crisis. Medical units see behavioral emergencies every day because medical illness changes behavior. A patient can be terrified and dangerous without being “psychiatric” in the narrow sense many teams use.
A useful bedside habit is to name the problem by function, not label. “Acutely agitated and unsafe.” “Disorganized, fearful, and trying to leave.” That keeps the team focused on observable risk.
Practical rule: In the opening minutes, treat behavior as a safety issue and a clinical clue at the same time.
The broader system has changed too. The 988 Suicide & Crisis Lifeline launched in July 2022 and handled almost 5 million contacts in its first year, a 40% increase over the previous system. By March 2024, average wait time was 21 seconds, showing how much demand exists for rapid behavioral health support at scale. That matters inside hospitals because it reflects a larger shift. Crisis care is no longer built around “send everyone to the ED and hope for the best.”
Early signs staff often miss
Escalation rarely starts with shouting. It often starts with scanning the room, refusing simple care, sudden guardedness, pacing, clenched jaw, or fixation on one false belief. If you want a quick public-facing summary of common indicators of mental health emergency, that resource is useful for orienting newer staff and families.
For staff communication, keep it concrete:
- State the observation: “He's getting more suspicious and is no longer redirectable.”
- State the risk: “He's moving toward the exit and pushing staff away.”
- State the need: “We need a lead speaker, environmental control, and medical assessment now.”
If difficult patient interactions are already straining your unit, these expert tips for dealing with difficult patients help reinforce the difference between routine conflict and a true crisis trajectory.
Conducting Rapid Triage and Risk Assessment
A crisis assessment isn't a full psychiatric interview. It's a fast safety screen that answers one question: what can hurt this patient or someone else in the next few minutes or hours?
Roberts' seven-stage crisis model puts biopsychosocial and lethality assessment first, with explicit priority on suicidal and homicidal risk, substance use, and medical needs before deeper problem-solving begin.
Start with the things that kill first
Think in layers. Airway and oxygenation still matter. So do glucose, stroke symptoms, head injury, sepsis, intoxication, and withdrawal. If the behavior is new, abrupt, fluctuating, or paired with altered attention, suspect a medical driver until you've ruled it out.
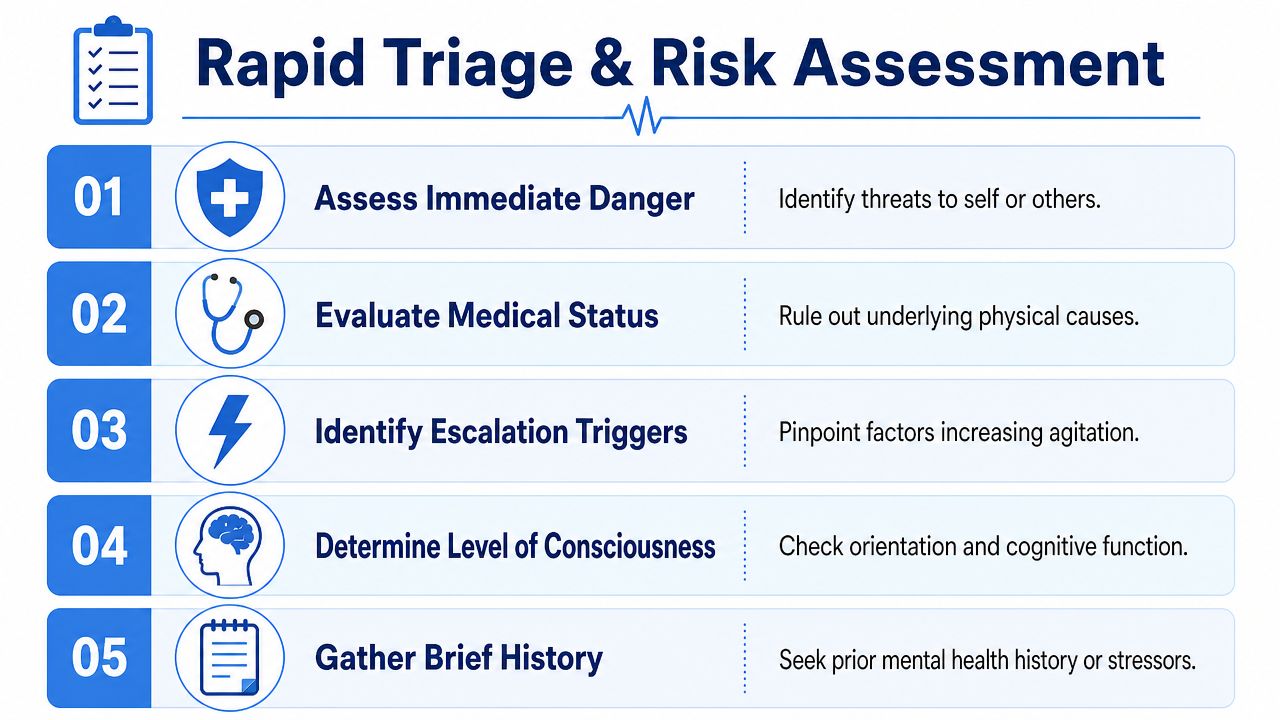
Use a short bedside sequence:
- Immediate danger
Is the patient attempting self-harm, threatening others, grabbing equipment, or trying to elope into unsafe space? - Medical status
Check for distress, abnormal vitals, pain, hypoxia, hypoglycemia, fever, medication effects, or acute neurological change. - Consciousness and orientation
Are they alert, confused, inattentive, disorganized, or unable to track a simple question? - Lethality
Ask directly about suicide, homicide, command hallucinations, intent, means, and recent acts. - Substance and withdrawal
Look for intoxication, stimulant use, alcohol withdrawal, sedative withdrawal, or mixed presentations.
Questions that are brief and useful
Don't hide behind vague phrasing. Direct questions are safer.

A patient can deny suicidal intent and still be high risk because of disorganization, inability to care for basic needs, severe impulsivity, or command hallucinations. Clinical judgment still matters.
When the story and the presentation don't fit, slow down and look for a medical cause.
Common triage errors
New clinicians often make the same mistakes:
- They overtalk. A distressed patient won't give you a clean history if you ask five-part questions.
- They assume behavior equals intent. Agitation may reflect fear, pain, delirium, trauma, or withdrawal.
- They skip collateral. Family, EMS, previous notes, and bedside staff often hold the missing detail.
- They chart labels instead of findings. “Combative” is less useful than “struck bedrail, pulled IV, advanced toward staff despite redirection.”
For clinicians who want to sharpen the assessment side of this work, these patient assessment tips for paramedics translate well beyond prehospital care because they reinforce prioritization under pressure.
Mastering Verbal and Environmental De-escalation
Once you've checked for immediate medical and violence risk, your next task is to reduce arousal without increasing shame or confrontation. De-escalation isn't about controlling another person. It's about giving the nervous system fewer reasons to keep escalating.
The fastest way to lose the room is to sound rushed, authoritative, or dismissive. Patients in crisis often hear threat before they hear content. Your tone, spacing, posture, and pacing all communicate before your words do.
What to say and what to avoid
A good de-escalator sounds steady, brief, and respectful.
Try language like:
- Acknowledge emotion: “You seem scared and overloaded right now.”
- Offer help without force: “I want to help you get through this safely.”
- Set one limit clearly: “I can talk with you, but I can't let anyone get hurt.”
- Give simple choices: “Would you rather sit in the chair or stand by the door while we talk?”
Avoid lines that trigger a power struggle:
- “Calm down.” Patients usually hear this as criticism.
- “If you don't cooperate…” Threats raise the stakes.
- “That makes no sense.” Logic challenges don't calm psychosis or panic.
- “You're fine.” Reassurance that ignores distress feels false.
Use validation without agreeing to unsafe beliefs
Validation means you recognize the person's internal experience. It doesn't mean you confirm delusions, endorse violence, or argue over reality.
A helpful formula is:
- Feeling: “It sounds like you feel trapped.”
- Need: “You want more control over what happens next.”
- Boundary: “We can work on that safely.”
That middle step matters. Patients settle faster when they're offered a path that preserves dignity.
Here's a useful teaching aid for emotional regulation skills that can support post-crisis coaching and patient education: Refresh Psychiatry's DBT skills guide. DBT language often helps staff frame distress as something that can be managed, not fought.
The room is part of the intervention
Environmental de-escalation is often neglected because people focus on the script. But the setting can either lower the temperature or keep feeding it.
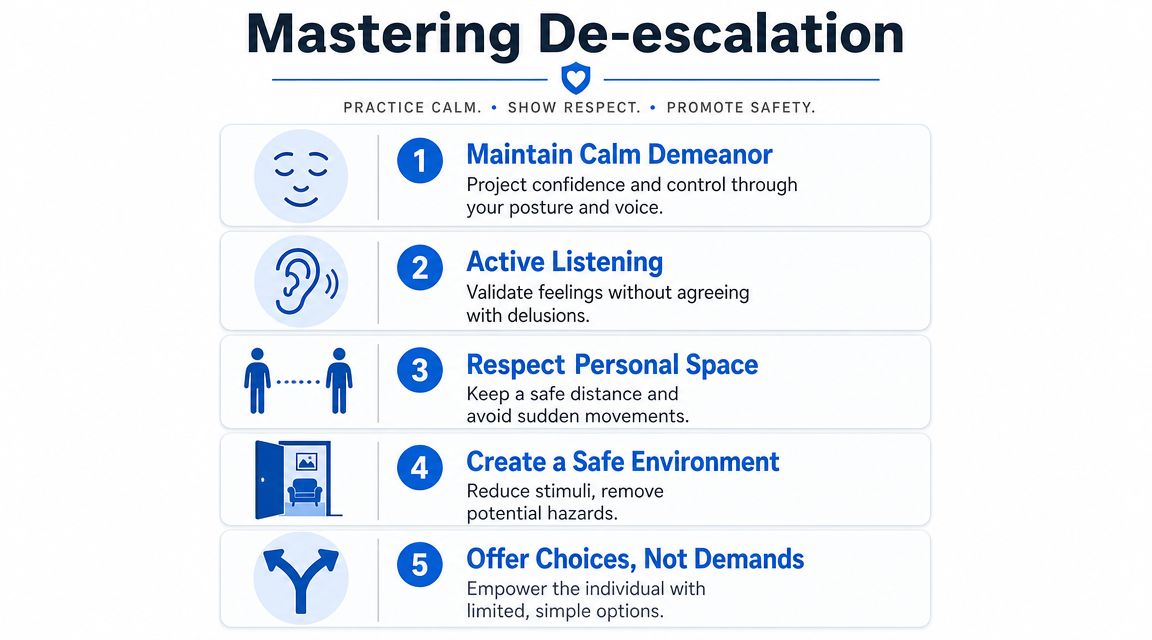
Use this checklist:
- Reduce stimulation: Lower TV volume, silence unnecessary alarms if clinically appropriate, and limit bystanders.
- Preserve exits: Don't block the patient's path to the door, and don't trap yourself either.
- Watch your body language: Keep hands visible, stance open, and movements predictable.
- Remove hazards: Sharps, cords, heavy objects, and loose equipment shouldn't stay within reach.
- Assign roles: One lead speaker, one safety backup, one medication or equipment runner if needed.
“Slow is smooth, smooth is fast” applies here. A measured approach often prevents the need for force later.
De-escalation is influence, not surrender
Some clinicians worry that offering choices means giving up control. It doesn't. You're shaping the interaction so the patient can regain enough control to participate safely.
There's also a limit. If the patient can't process language, keeps advancing, or becomes imminently dangerous, verbal strategies alone may no longer be enough. Good de-escalation includes recognizing when it has stopped working.
When to Implement Advanced Safety Measures
There are times when the least restrictive approach still isn't enough. A patient may be actively trying to strike staff, rip out life-sustaining lines, run into traffic, or act on suicidal intent. In those moments, advanced safety measures can be necessary. They should never be casual, punitive, or convenience-based.
The threshold for escalation
Use restrictive measures only when there is imminent risk of harm and less restrictive options have failed or are not feasible. That includes situations where the patient's behavior creates immediate danger to self or others, or where severe disorganization makes basic safety impossible.
A practical decision frame looks like this:
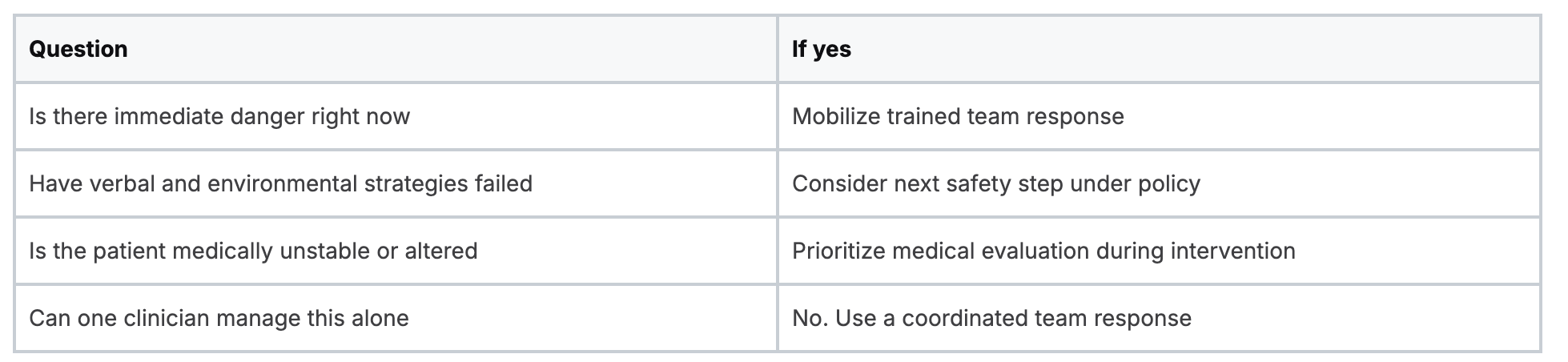
Team response matters
No one should improvise restraints alone. The safest responses are structured, role-based, and policy-driven. One person leads communication. Others manage limbs or equipment only if the team moves to that stage and only according to training and facility protocol.
If medication is used for behavioral emergency, the same rule applies. It must be tied to safety, clinical judgment, and monitoring. Sedation is not treatment for staff frustration.
Key guardrails:
- Use the least restrictive option available
- Explain what is happening, even if the patient is highly agitated
- Monitor continuously for respiratory, circulatory, and psychological distress
- Reassess often and discontinue as soon as it is safe
Ethical and legal responsibilities
The legal record starts before the restraint order. It begins with your observations, alternatives attempted, risk rationale, team communication, and ongoing reassessment. If your documentation reads like punishment or convenience, it will be hard to defend because it should be.
Safety measures are justified by danger, not by defiance.
Clinicians also need to remember the emotional aftermath. Many patients experience restraint as terrifying, humiliating, or traumatic, even when it was clinically necessary. Debriefing and follow-up aren't optional extras. They are part of ethical care.
Creating a Brief Intervention and Safety Plan
Once the patient is no longer escalating, the work changes. You're no longer just containing risk. You're helping the patient leave the encounter with a short, usable plan.
Many crisis responses frequently fall short. Staff feel relief once the room is calm, but calm isn't the endpoint. The patient still needs a bridge through the next day or two.
Keep the plan concrete and short-term
A brief safety plan should fit real life. Not ideal life. Real life.
Focus on the next 24 to 48 hours in practical terms:
- Warning signs: What tells the patient they're escalating again?
- Internal coping steps: What can they do on their own for the next few minutes?
- People and places: Who can they contact, and where can they go that feels safer?
- Professional support: Which service, clinic, team, or line should they use if the crisis returns?
- Means safety: What needs to be limited or handed off to reduce immediate danger?
Write it in the patient's own language when possible. “Take a walk and call my sister” works better than “utilize support network.”
Collaboration works better than instruction
Patients are more likely to use a plan they helped build. Ask for one step they believe they can do, not the step you think sounds best. Agency matters in crisis recovery because the person has usually just lived through a period of feeling powerless.
A simple bedside script can help:
- “What usually tells you things are getting bad?”
- “What has helped even a little in the past?”
- “Who is one person you'd answer if they called?”
- “What should happen next if tonight gets worse?”
Data supports this stepped approach. In one summary of crisis system outcomes, 78% of 988 or crisis contact center contacts were resolved without additional interventions, and mobile crisis teams resolved 72% without needing escalation to more intensive services, according to the NRI report on behavioral health crisis system outcomes. Those numbers don't mean every crisis is simple. They do show that focused intervention, good triage, and strong linkage often keep people out of more restrictive settings.
What a good plan is not
It is not a lecture. It is not a stack of discharge papers with no human explanation. It is not “follow up with psych” written in a chart while no appointment, contact pathway, or family support has been clarified.
A useful safety plan is brief, visible, and specific. If the patient can't repeat it back in plain language, it's probably too vague to hold under stress.
Handoff, Documentation, and Continuing Education
A calm patient can still have a dangerous transition. Poor handoff is where information disappears, risk gets diluted, and preventable returns begin. Good mental health crisis intervention includes the next clinician, the next setting, and the next contact.
SAMHSA and NAMI frame crisis care as a continuum that includes hotlines, mobile teams, stabilization, and follow-up, not just the initial response, as described in SAMHSA's national behavioral health crisis care guidance. That same mindset should shape your bedside handoff.
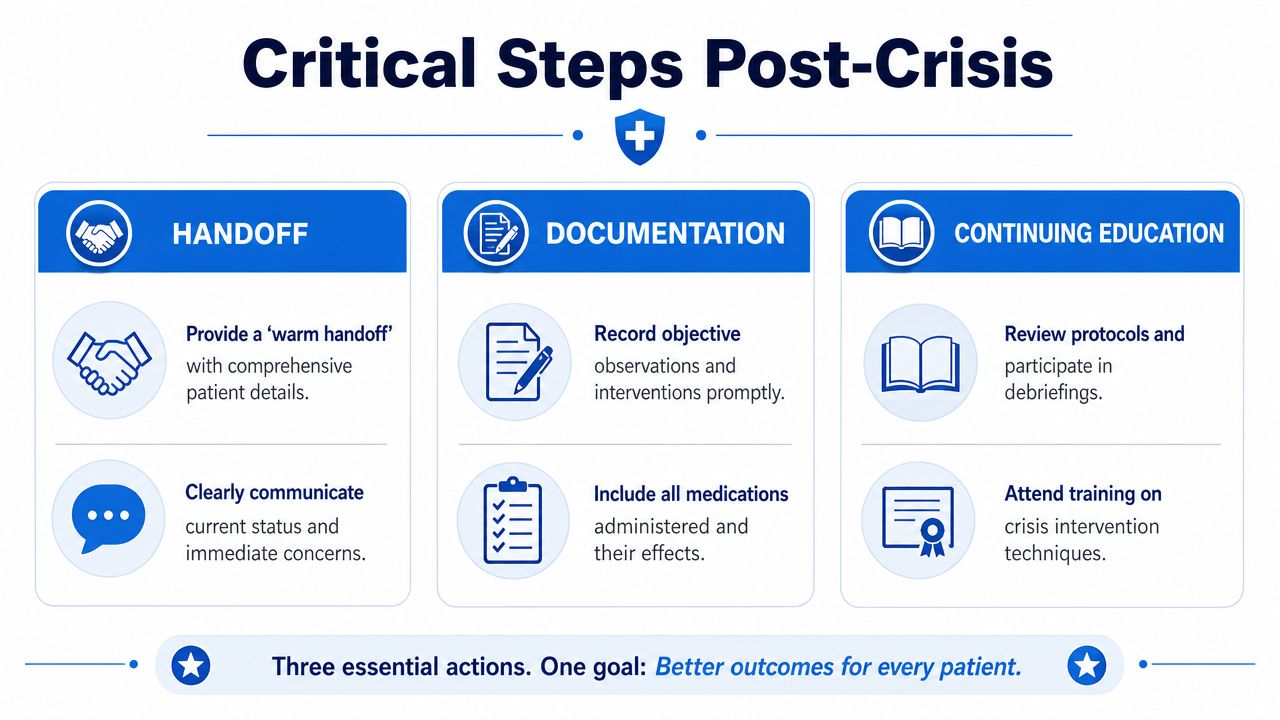
What a warm handoff sounds like
A weak handoff says, “Behavioral issue. Better now.”
A strong one includes:
- Observed behavior: what the patient did, not just the label used
- Risk findings: suicide, violence, psychosis, confusion, elopement, refusal, means access
- Medical context: recent surgery, new meds, intoxication concern, hypoxia concern, delirium concern
- Interventions and response: what you tried, what helped, what didn't
- Current status: calm, guarded, asleep, cooperative, disorganized, still high risk
- Next step: exact service or team receiving responsibility
Documentation protects care and clinicians
Chart facts, sequence, and rationale. Avoid loaded language and hindsight logic. If you offered choices, documented direct risk questions, consulted the right people, and reassessed after interventions, your note should show that clearly.
Useful documentation habits:
- Be objective: “Patient shouted that staff were trying to kill him and swung right arm toward nurse.”
- Track alternatives attempted: verbal redirection, reduced stimuli, support person contacted, medical review initiated
- Record response: improved, unchanged, worsened, intermittently redirectable
- Include follow-up arrangements: handoff recipient, disposition, instructions, safety plan elements
Healthcare leaders also think about crisis response as an operational risk issue, not just a clinical one. For organizations examining system vulnerabilities around access, continuity, and reimbursement pressure.
Why continuing education matters, and why online training counts
Behavioral crises don't show up on a convenient schedule. Staff need training they can complete, revisit, and apply. That's one reason accredited online education keeps gaining ground across healthcare. The old assumption that only in-person classes from a narrow set of organizations are acceptable no longer reflects how many hospitals, clinics, and professional teams handle education.
What matters is quality, accreditation, relevance, and whether the training improves bedside performance. Online formats give clinicians flexibility, repeat exposure, and easier access for recertification and CE. For busy professionals, that often means better follow-through, not less rigor.
If you're reviewing options for maintaining competency, online continuing medical education is a practical place to start. Modern healthcare education has moved well beyond the idea that credibility depends on being in a classroom seat.
Training should fit clinical reality. If a format helps clinicians learn, retain, and return to the bedside prepared, it belongs in the conversation.
Strong crisis care depends on what you do before the room escalates, while the patient is escalating, and after the patient appears calm. If you want a flexible way to build those skills alongside your required certifications and continuing education, ProMed Certifications offers accredited online training designed for healthcare professionals who need credible, practical education that fits real schedules.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)
.png)