Code Silver Hospital Meaning: Active Shooter Response

You’re documenting meds, answering a call light, and trying to stay on schedule. Then the overhead speaker cuts in with a calm, clipped announcement: Code Silver.
That moment can feel like the floor drops out from under the shift. Even experienced clinicians can freeze for a second, not because they don’t care, but because high-stakes alerts scramble normal thinking. In a hospital, where patient care usually drives every decision, a Code Silver changes the priority fast. Safety comes first.
The good news is that this response can be learned, practiced, and remembered. The code silver hospital meaning isn’t vague once you break it down into plain actions. When you understand what the code means, what your job is, and how your facility responds around you, you’re much more likely to act decisively under stress.
What to Do When Your Shift Is Interrupted by a Code Silver
A common scenario looks like this: a nurse is charting at the station, a respiratory therapist is moving between rooms, and a physician is discussing a plan with family. Then the intercom announces, “Code Silver, Emergency Department.”
The first reaction is usually not polished. It’s human. Your heart rate jumps, your attention narrows, and your brain starts asking rapid questions. Where is it? Is it near me? Do I move patients? Do I lock down? Do I call someone first?
That uncertainty is exactly why Code Silver training matters. In a real emergency, nobody gets extra time to look up policy. You act from what you already know.
Practical rule: In the first seconds of a Code Silver, don’t chase perfect information. Focus on your immediate safety decision.
If you work in emergency medicine or another fast-moving unit, the emotional strain of these alerts can linger long after the announcement ends. Stress management is part of professional readiness, not a side issue. Resources on coping with stress in emergency medicine can help you prepare mentally before a crisis ever happens.
The first mental reset
When the code is called, switch from routine care mode to threat-response mode.
Ask yourself:
- Where is the threat reported: Is it in your area or far from you?
- What patients are with me right now: Who can move quickly, and who can’t?
- What’s my nearest safe option: Exit, secure room, or barricade point?
That simple reset helps cut through panic. You don’t need to know everything at once. You need to make the next safe decision.
The Official Meaning of Code Silver in a Hospital
Code Silver means there is an active shooter, a person with a weapon, or a hostage situation in the hospital. That is the core code silver hospital meaning used in many healthcare settings, and it’s one of the most serious alerts a facility can issue, based on the Louisiana Hospital Association sample policy.

This is different from a generic behavior problem. A loud, angry, or combative person may trigger a different code in your facility. Code Silver signals something more dangerous. A weapon is confirmed or strongly suspected, or there is an active assailant situation.
Why hospitals use this code
Hospitals developed emergency codes so staff could communicate urgent threats quickly without creating unnecessary confusion for patients and visitors. Code Silver became a critical part of that system as healthcare organizations recognized violence risk in hazard vulnerability reviews and emergency planning.
The reason the code matters is simple. It shifts the goal of your response.
In most hospital emergencies, your first instinct is to move toward the patient and provide care. In a Code Silver, the first job is survival and protection. Clinical care may pause because the immediate threat has to be addressed first.
What the announcement triggers
When Code Silver is called, it activates the run, hide, fight protocol described in hospital policy guidance.
That means:
- Run if it’s safe to evacuate: If you have a clear path away from danger, leave.
- Hide if you can’t leave safely: Secure yourself and patients in a protected space, barricade if possible, and silence devices.
- Fight only as a last resort: If the attacker reaches you and escape or concealment is no longer possible, use available objects to defend yourself.
A Code Silver isn’t a signal to “wait and see.” It’s a signal to choose a survival action immediately.
Why readers often get confused
A lot of confusion comes from the fact that codes vary between facilities and regions. In many hospitals, Code Silver is closely tied to weapon threats. In some places, plain-language alerts are replacing color codes altogether because they’re easier to understand in the moment.
That’s why staff who travel, float, or move between systems should never assume every hospital uses the same wording. The safest approach is to know the broad meaning of Code Silver and also learn your facility’s exact policy, overhead language, and reporting process.
A useful way to remember it is this: Code Blue means save a patient. Code Silver means first save yourself and those immediately around you from an armed threat.
Your Role During a Code Silver Run Hide or Fight
Your role during a Code Silver is personal, immediate, and practical. You’re not expected to solve the whole event. You’re expected to make the safest choice available where you are.

Run when you can
If there is a safe path away from the threat, leave. Don’t stop to collect your bag, phone charger, or jacket. Those are replaceable.
If patients or visitors can move with you safely, direct them quickly and clearly. Use short commands. “Come with me.” “Stay low.” “This way.”
A good mental model is a fire alarm with a different cause. You’re not evacuating because of smoke. You’re evacuating because staying in place is more dangerous than leaving.
Key reminders:
- Move away from the threat: Don’t head toward the announced location.
- Use familiar exits: Staff exits, stairwells, and secondary paths matter.
- Keep instructions simple: People process less under stress.
Hide if leaving isn’t safe
If evacuation would put you in more danger, hide. In a hospital, that usually means turning a room into a temporary shelter.
Do what you can, quickly:
- Lock or barricade the door: Beds, carts, chairs, and wedges can help.
- Silence devices: Phones, pagers, and alarms can reveal your location.
- Reduce visibility: Lights off, blinds closed if possible, stay away from doors and windows.
- Protect immobile patients: Move them out of direct sight if you can do so safely.
Think of hiding as buying time. You’re trying to make your room hard to access, hard to hear, and hard to see into.
If you can’t leave, make the room feel occupied by no one and difficult to enter.
Fight only if there is no other option
This is the part people often struggle with because it feels out of character for healthcare work. But fighting in this context is not aggression for its own sake. It is last-resort survival.
If the attacker is in your space and you have no safe way out, commit to disrupting the threat. Use whatever is available. A fire extinguisher, IV pole, chair, sharps container, or heavy equipment can become an improvised defensive tool.
The goal is not to “win” in a conventional sense. The goal is to create enough disruption to stop the attacker's control and improve your chance of survival.
A short visual refresher can help fix the sequence in memory:
What if you’re with patients
Healthcare professionals feel the most internal conflict. You care for vulnerable people. But during an armed threat, you can’t help anyone if you become a victim yourself.
Use this order of thinking:
- Protect yourself first
- Take patients with you if it’s immediately safe
- Secure immobile patients in place if evacuation isn’t realistic
- Follow law enforcement instructions once they arrive
That may feel harsh. It’s disciplined. In a Code Silver, survival decisions have to be made fast and without guilt-driven hesitation.
How Your Facility Responds to a Code Silver Alert
While you’re securing yourself and your patients, the rest of the hospital is shifting into a coordinated emergency response. The response can feel chaotic from inside a locked room, but the system behind it is designed to be structured.
According to a Dignity Health code guide, Code Silver protocols focus on rapid lockdown and perimeter control. Integrated systems can support containment within 60 to 90 seconds, activation can notify dozens of response personnel, and access controls may lock 80% to 95% of access points to limit movement and spread of the threat, as described in the Dignity Health emergency color codes document.
What happens behind the scenes
Once the alert is activated, several things usually happen at once:
- Security is mobilized: Internal teams move to preassigned roles.
- Law enforcement is contacted or integrated: The hospital shares location details as quickly as possible.
- Entrances and corridors are controlled: The goal is containment, not random movement.
- Staff receive updates: Overhead paging, phones, or message systems may relay new information.
This is why the distinction between Code Silver and a non-weapon violence code matters. The armed-threat response is built for a very different risk profile.
Why access control matters
Hospitals are difficult environments to secure. They’re open, busy, and full of vulnerable people. A Code Silver response depends heavily on who can close doors, monitor movement, and restrict entry without delaying critical communication.
For facilities reviewing these systems, tools that modernize building access can be useful to explore because they show how credentialing, visitor access, and entry management can support clearer building control during emergencies.
Staff often think a Code Silver response is only about personal actions. It’s also about whether the building itself can help protect the people inside it.
What this means for you in the moment
Your facility’s response plan is meant to reduce the number of decisions you have to make under pressure. If doors lock, units seal, and information flows to the right people, you can stay focused on your immediate environment.
That doesn’t remove stress. It does reduce confusion.
A practical takeaway is to learn your hospital’s activation process before you need it. Know the emergency number, know how your unit receives alerts, and know which doors around you lock manually versus electronically. Those details matter more than one might realize until the day they need them.
Code Silver vs Other Hospital Emergency Codes
One reason the code silver hospital meaning gets misunderstood is that hospital code systems are not perfectly uniform. Some meanings overlap. Some facilities rename codes. Others switch to plain language because they want fewer interpretation errors.
A source discussing code variation notes that Code Silver commonly refers to a weapon threat, active shooter, or hostage situation in many settings, but meanings can vary by region and institution. It also notes that over 20% of facilities customize codes, which raises confusion risk, and that some organizations are moving toward plain language or numeric systems.
The most important comparison
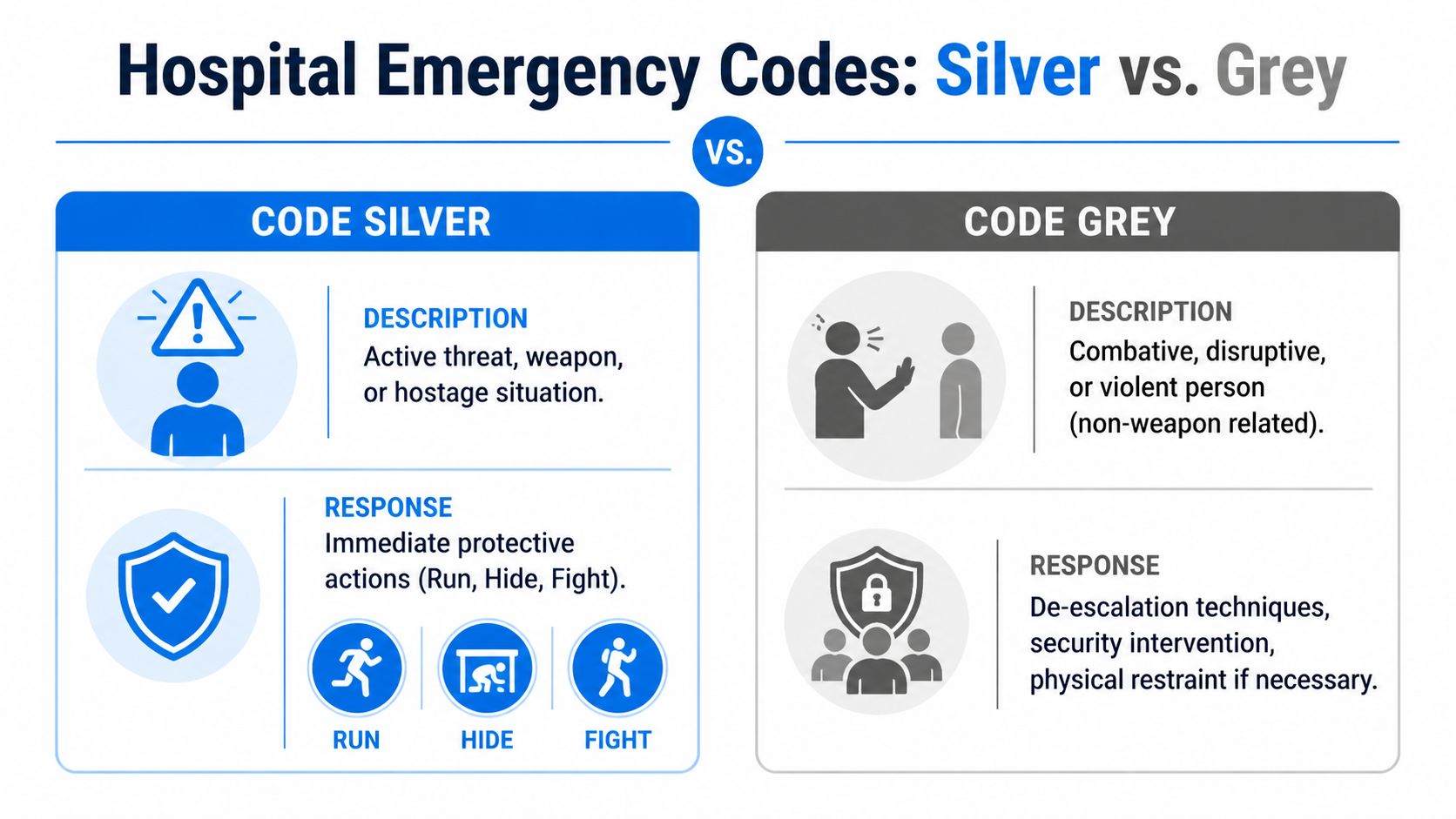
The easiest mix-up is Code Silver vs Code Grey.
Here’s the quick distinction:
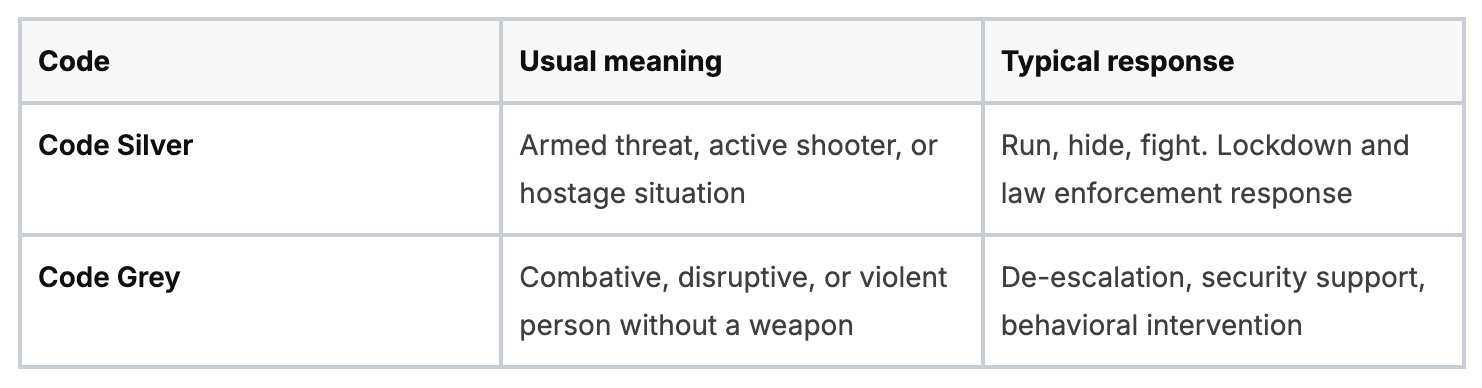
That difference changes everything. In a Code Grey, staff may call for trained assistance and use de-escalation strategies. In a Code Silver, you don’t stay close to talk someone down if there is an active weapon threat. You protect life through distance, concealment, and last-resort defense.
Other common code overlaps
A few other codes cause confusion because names and meanings differ between hospitals.
- Code Red: Usually fire. That response focuses on fire safety and containment. If you need a refresher, this guide on Code Red hospital emergency training and what you'll learn helps clarify how different that workflow is from an armed-threat response.
- Code White: In some systems this refers to a violent person. In others, it can mean something completely different.
- Code Black: Often a bomb threat, though not universally.
Why plain language is gaining ground
A color code works only if everyone knows exactly what it means. That becomes harder when staff travel, float between campuses, or work in mixed systems.
Plain-language alerts solve a practical problem. “Active shooter in the Emergency Department” leaves less room for interpretation than a code that might mean different things somewhere else.
Clear language beats familiar language if familiar language creates hesitation.
What to do if you work in more than one facility
If you pick up shifts in different places, don’t rely on memory from your home hospital. Ask for the emergency code list during orientation. Keep it accessible until you know it cold.
Focus on three questions:
- Which code means armed threat here
- How is the alert delivered
- What does this unit expect staff to do first
That small habit prevents one of the biggest avoidable errors in emergency response. Assuming your current facility uses the same system as the last one.
Essential Training and Preparedness for Hospital Emergencies
Preparedness is often thought to start with memorizing a code. It doesn’t. Real preparedness starts when you can hear the alert, feel the adrenaline, and still move into the correct action.
Hospital code systems have changed over time. The first Code Blue was used at Toronto General Hospital in 1958, and hospital emergency code systems have since expanded to 10 to 20 or more codes used in thousands of facilities. Some analyses cited in the overview of hospital emergency codes describe healthcare workplace violence as rising 400% from 2000 to 2020, and note that over 70% of hospitals use Code Silver.

That evolution tells us something important. Emergency preparedness in healthcare can’t stay static while threats change.
What good preparedness actually looks like
Strong readiness has a few parts working together:
- Policy knowledge: You know your facility’s code language, reporting route, and lockdown expectations.
- Mental rehearsal: You’ve already thought through exits, secure rooms, and patient movement on your unit.
- Skills practice: You’ve drilled enough that your response isn’t your first time thinking through it.
- Recovery awareness: You understand that post-incident reporting, debriefing, and emotional support are part of professional practice too.
Many facilities also review building design, entry control, and security staffing as part of preparedness. For teams interested in healthcare-focused physical protection planning, resources on Securitec healthcare security can offer useful examples of how clinics and healthcare offices think about access, surveillance, and threat reduction.
Why online training deserves to be taken seriously
There’s still an outdated belief in some circles that only in-person programs count, especially if they come from a narrow list of legacy organizations. That belief doesn’t match where healthcare education is heading.
Online education is now a normal part of how clinicians maintain competence. It fits rotating schedules, night shifts, family demands, travel assignments, and multi-site work in a way classroom-only models often can’t. For CE and certification prep, accessibility matters because training only works if busy professionals can complete it well.
That doesn’t mean quality should drop. It means quality has to be designed well.
Good online healthcare training gives you:
- Flexible pacing: You can revisit difficult concepts instead of pretending you understood them in a live room.
- Repeat exposure: Reviewing scenarios more than once strengthens recall under stress.
- Less logistical friction: No commute, no classroom scheduling bottleneck, no loss of a full workday.
- More consistent delivery: Every learner gets the same core material.
The question isn’t whether learning happens online. The question is whether the course is accurate, accredited, and built for real clinical decision-making.
Training should match how healthcare work actually happens
A nurse on a twelve-hour shift, a physician between patient loads, and a travel clinician onboarding to a new system all need training that respects time constraints without lowering standards. That’s one reason online CE and certification formats are gaining wider acceptance across hospitals, clinics, and healthcare organizations.
What matters most is whether the training helps you perform. If you can identify the threat, choose between run, hide, or fight, secure patients appropriately, and function within your facility’s response plan, the format has done its job.
Practical emergency readiness also benefits from team-based preparation. If your workplace is reviewing unit roles, command structure, and coordinated drills, this resource on emergency response team training is a useful companion.
The confidence piece people overlook
Competence and confidence are not the same thing, but they reinforce each other. Staff who have practiced emergency responses tend to move faster, communicate more clearly, and recover their focus sooner.
You do not need to become fearless to be effective in a Code Silver. You need a plan that is simple enough to hold under pressure and familiar enough to act on quickly.
That is why regular refreshers matter. Not because you’ll use them every day, but because if the day comes, you’ll need them immediately.
Preparedness is part of patient safety, colleague safety, and your own safety. If you need flexible, accredited training that fits real healthcare schedules, ProMed Certifications offers online certification and continuing education designed for working clinicians who need convenience without sacrificing credibility.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)