CPAP and Congestive Heart Failure
.png)
A familiar scenario plays out on rounds. Your patient with congestive heart failure is taking guideline-directed medical therapy, watching sodium, weighing daily, and still waking exhausted, short of breath, and foggy. The edema is better. The medication list looks solid. Yet something still isn’t adding up.
Often, the missing piece is happening while the patient sleeps.
In heart failure care, sleep-disordered breathing is easy to under-recognize because its clues overlap with CHF itself. Fatigue, morning headaches, nocturnal dyspnea, fragmented sleep, poor exercise tolerance, and resistant blood pressure patterns can all blur together. If we only focus on the daytime cardiology picture, we can miss a major driver of overnight physiologic stress.
That’s where the conversation about cpap and chf becomes clinically important. CPAP is not merely a comfort device for snoring. In the right patient, it can change oxygenation, sympathetic tone, intrathoracic pressure, and cardiac workload in ways that matter. It can also fail if we apply it to the wrong phenotype, use the wrong pressure strategy, or ignore adherence barriers.
For busy clinicians, this is exactly the kind of topic that benefits from high-quality online education. You don’t need to sit in a hotel conference room to learn modern cardio-sleep management well. Online CE and certification formats now give clinicians a practical way to stay current, review cases, and revisit difficult concepts on demand. That’s especially useful in an area like heart failure and sleep medicine, where nuances matter and protocols keep evolving. The old idea that only a narrow set of in-person classes counts is outdated.
An Introduction to CPAP and Congestive Heart Failure
CHF and sleep apnea often travel together, but they don’t behave the same way in every patient. Some patients have obstructive sleep apnea, where the upper airway collapses despite respiratory effort. Others have central sleep apnea, where ventilatory drive becomes unstable. In heart failure, that central pattern may appear as Cheyne-Stokes respiration, the waxing and waning breathing pattern many of us recognize on telemetry or a sleep study.
That distinction matters because CPAP is not a generic answer to “bad sleep” in heart failure. It’s a targeted therapy. When it matches the underlying breathing disorder, it can reduce nightly physiologic stress that standard daytime CHF treatment doesn’t fully address.
A good clinical habit is to ask three simple questions in any CHF patient with persistent symptoms:
- What happens at night
Does the patient snore, gasp, stop breathing, awaken choking, or sleep upright? - What happens in the morning
Are they waking unrefreshed, headachy, tachycardic, or hypertensive? - What remains unexplained
If symptoms seem disproportionate to the exam, echo, and medication regimen, sleep-disordered breathing should move up the list.
Why this shows up in everyday practice
Many CHF patients don’t complain of “sleep apnea.” They report poor sleep, nocturia, fatigue, or worsening dyspnea when lying flat. Family members may be the ones who notice the breathing pauses. In central patterns, there may be no loud snoring at all.
From a documentation standpoint, it also helps to code heart failure accurately when you’re coordinating referral, follow-up, and payer communication.
Clinical lens: If a CHF patient remains symptomatic despite reasonable medical optimization, don’t assume the remaining burden is only “advanced heart failure.” Nighttime breathing instability may be part of the problem.
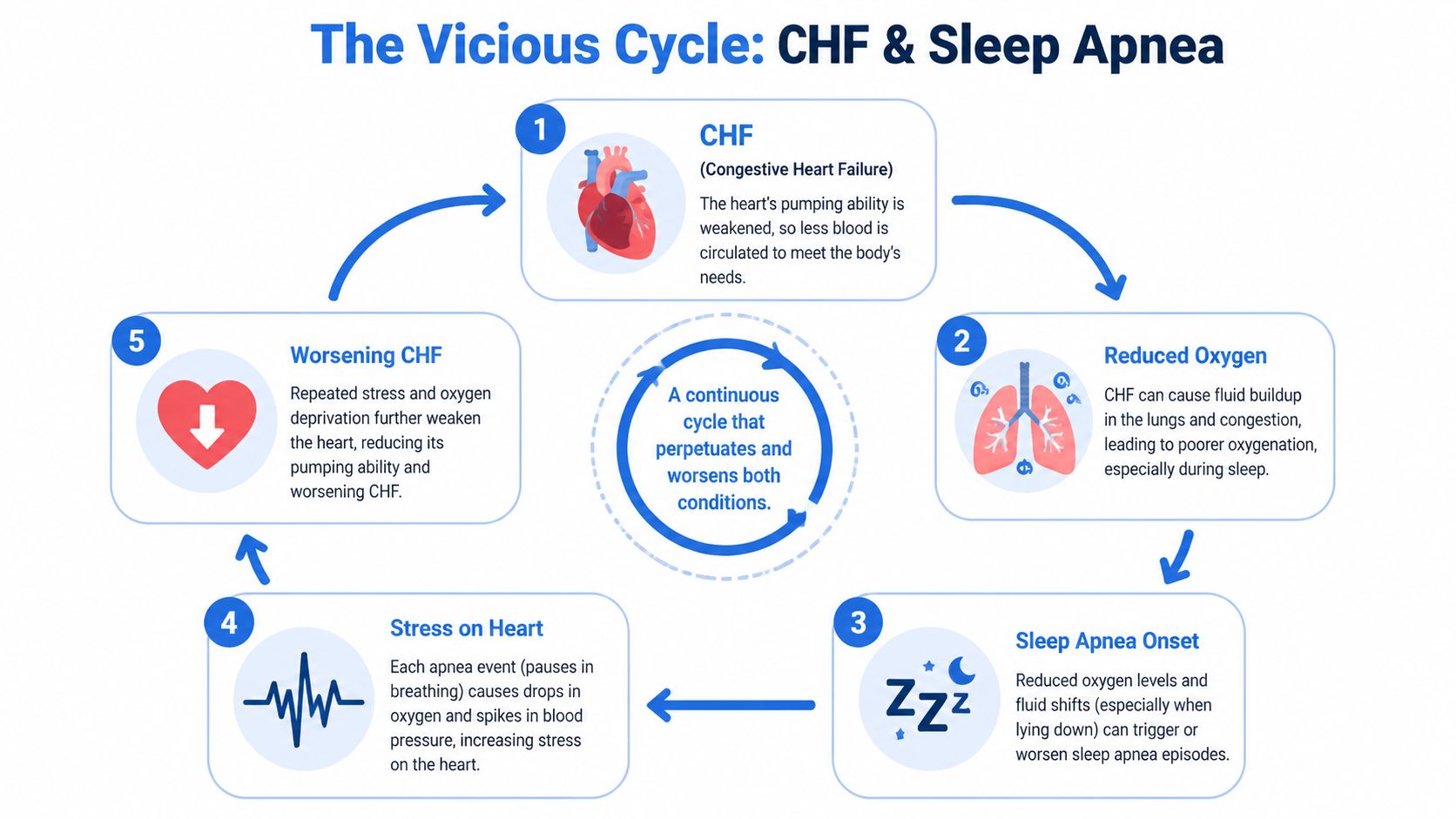
The Vicious Cycle of CHF and Sleep Apnea
Heart failure and sleep apnea reinforce each other. That’s the simplest way to understand the relationship.
A weakened ventricle changes filling pressures, pulmonary hemodynamics, and gas exchange. Overnight, those changes can destabilize breathing. Then each apnea event adds more stress back onto the heart. The cycle repeats for hours.
How heart failure sets up sleep-disordered breathing
In CHF, fluid doesn’t just stay in the legs. When a patient lies down, fluid redistribution can worsen upper-airway narrowing and increase pulmonary congestion. At the same time, prolonged circulation time and unstable carbon dioxide control can make breathing more erratic. In some patients, that produces central apnea with the classic crescendo-decrescendo pattern of Cheyne-Stokes respiration.
Think of the respiratory control system as a thermostat that has become overly sensitive and slow to correct. The patient overbreathes, carbon dioxide drops, ventilatory drive falls, apnea occurs, carbon dioxide rises again, and the cycle restarts. A failing heart makes that instability more likely.
How apnea pushes back on the heart
Each apnea event is not just a sleep disturbance. It’s a cardiovascular event.
During repeated breathing pauses, patients experience:
- Intermittent oxygen drops that strain an already vulnerable myocardium
- Sympathetic surges that raise heart rate and blood pressure during the night
- Intrathoracic pressure swings that increase cardiac workload
- Fragmented sleep that leaves patients fatigued and less resilient during the day
This is why a patient can look “stable” by daytime metrics but still be under heavy physiologic stress every night.
Recurrent apnea acts like a series of small nocturnal stress tests that the failing heart never asked for.
Why untreated sleep apnea matters in heart failure risk
This relationship is not only theoretical. A Danish nationwide cohort study that followed 4.9 million individuals identified 40,485 patients who developed sleep apnea during the study period. In that study, untreated sleep apnea was associated with increased heart failure risk across age groups, and patients over age 60 who did not receive CPAP had a 38% higher risk of developing heart failure than those who used CPAP, according to the Danish cohort analysis of sleep apnea, CPAP use, and heart failure risk.
That finding aligns with what many clinicians already suspect from practice. Overnight respiratory instability is not a side issue in cardiovascular care. It can shape the trajectory of heart failure itself.
Where clinicians often get tripped up
The confusion usually comes from assuming all sleep apnea in CHF is obstructive. It isn’t. Obstructive and central events may coexist, but they have different mechanisms and often require a more careful read of the sleep study.
A quick patient-facing resource can also help when families ask basic screening questions before formal testing.
A practical bedside summary
The key point is simple. In cpap and chf, the “sleep problem” and the “heart problem” are often part of the same physiologic loop.
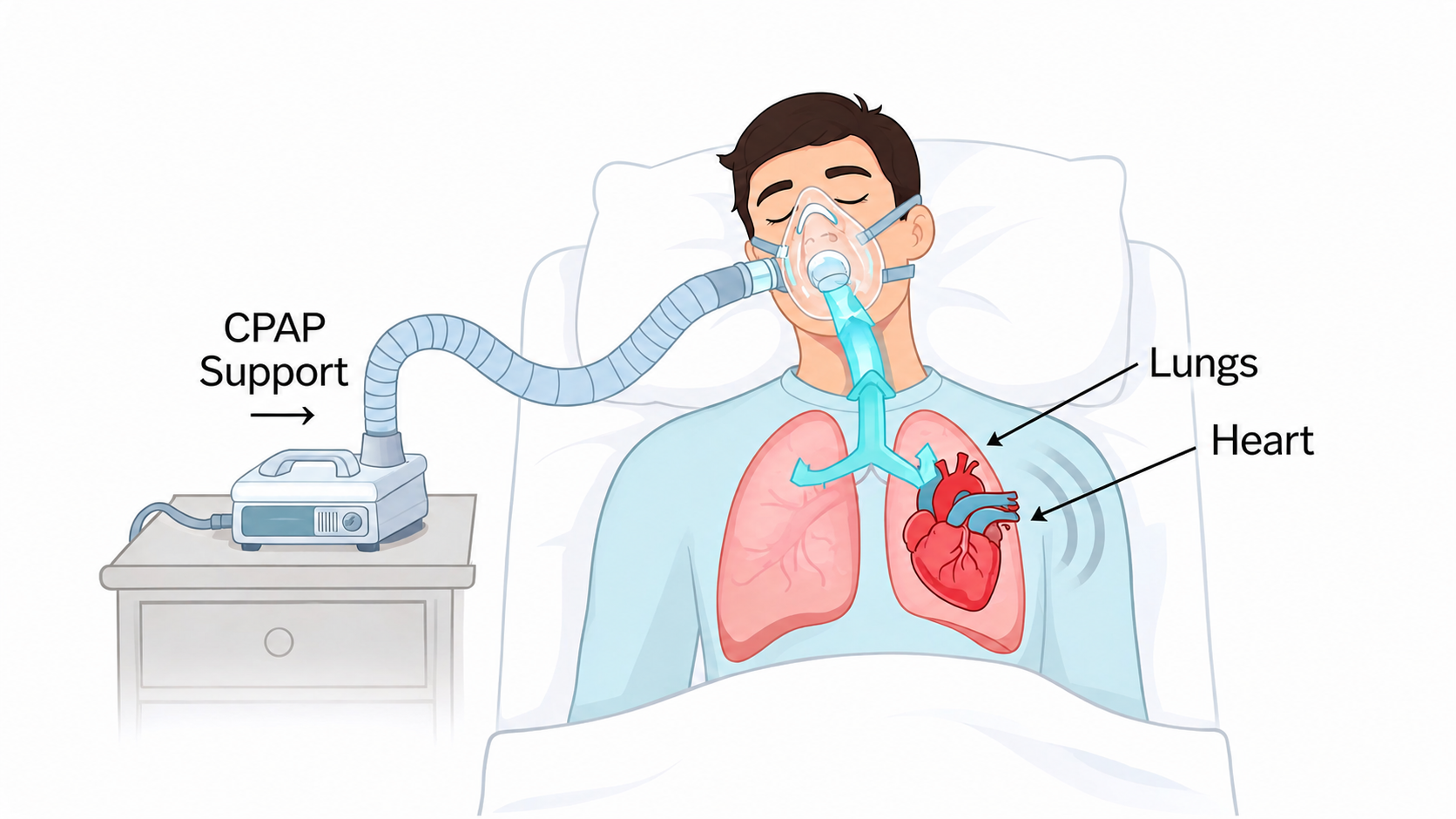
How CPAP Therapy Intervenes in Heart Failure
CPAP is often explained as a machine that holds the airway open. That’s true, but it’s incomplete.
In CHF, CPAP can act like a pneumatic splint for the airway and, in selected patients, a hemodynamic support tool. By applying continuous positive pressure, it can smooth out the nightly pressure swings that burden both the lungs and the heart.
What CPAP does mechanically
For obstructive events, the concept is straightforward. CPAP keeps the upper airway from collapsing. That prevents the stop-start pattern of airflow obstruction that leads to desaturation, arousal, and catecholamine release.
For the cardiovascular system, the pressure effect matters too. Positive airway pressure can reduce harmful negative intrathoracic pressure swings. In practical terms, that can lessen ventricular wall stress and reduce the amount of work the heart must do against changing pressures each night.
Why the heart may benefit
When CPAP works well in the right patient, several mechanisms move in the same direction:
- Improved oxygenation reduces nocturnal myocardial stress
- Less sympathetic activation lowers the repeated fight-or-flight surges associated with apnea
- Reduced afterload effects may make it easier for the left ventricle to eject blood
- More stable sleep architecture reduces recurrent arousals and physiologic volatility
If you need a quick refresher on the broader consequences of low oxygen states in acute and chronic illness, this review of hypoxia and its clinical effects helps connect the respiratory physiology to what we see at the bedside.
Where the best evidence is strongest
One landmark randomized trial is especially important for clinicians who manage heart failure patients with central patterns. In that study of 66 CHF patients, including 29 with CSR-CSA and 37 without, CPAP-treated patients with CSR-CSA who complied with therapy had an 81% relative risk reduction in the combined mortality-cardiac transplantation rate over a median 2.2-year follow-up. The same trial found a significant increase in left ventricular ejection fraction during the treatment period in the CSR-CSA group, as reported in the Circulation trial on CPAP in CHF patients with Cheyne-Stokes respiration and central sleep apnea.
That trial also gave us an equally important caution. CPAP did not show the same benefit in CHF patients without CSR-CSA. That’s why phenotype matters so much in cpap and chf. The therapy is not interchangeable across all heart failure patients.
Bedside takeaway: Don’t think of CPAP as “sleep equipment.” Think of it as targeted nocturnal cardiopulmonary therapy for the right breathing disorder.
A simple analogy that helps
If the failing heart is trying to pump while the chest generates repeated unstable pressure swings, CPAP can reduce some of that turbulence. It doesn’t replace diuresis, neurohormonal blockade, or rhythm management. It complements them by making the overnight environment less hostile.
That’s also why patients sometimes report benefits in ways that sound deceptively simple. They say they wake less panicked, need fewer pillows, feel less drained, or tolerate rehab better. Those comments often reflect meaningful physiologic improvement, even before you review the device data.
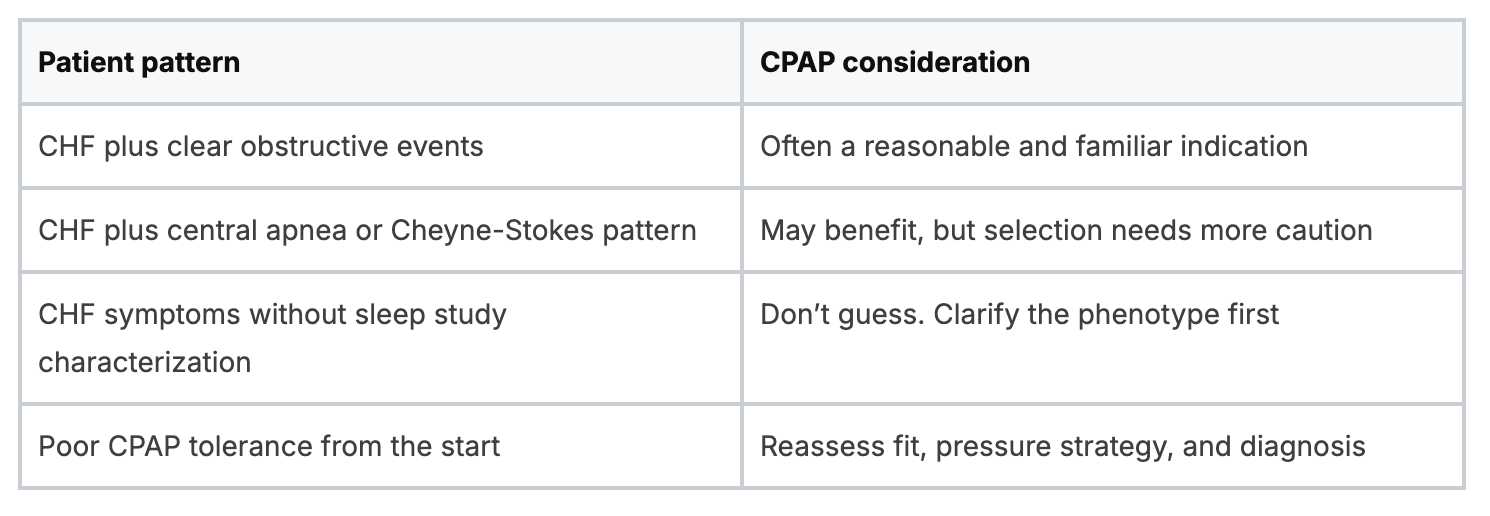
Key Clinical Indications for CPAP in CHF
The first question isn’t whether a CHF patient snores. The first question is what type of sleep-disordered breathing they have.
A practical way to think about CPAP indications in heart failure is to separate patients into two groups. One group has CHF with obstructive sleep apnea. The other has CHF with central sleep apnea, often with Cheyne-Stokes respiration. The overlap can be messy, but the categories help.
CHF with obstructive sleep apnea
These are the patients many clinicians recognize quickly. They may have loud snoring, witnessed obstruction, obesity, resistant hypertension, daytime sleepiness, and fragmented sleep. In this group, CPAP is often used because it prevents airway collapse and reduces the nightly cascade of desaturation and sympathetic activation.
The cardiovascular relevance goes beyond sleep quality. Consistent CPAP use of more than 4 hours per night in patients with OSA and cardiovascular disease, including CHF, is associated with a 31% lower risk of recurrent major adverse cardiovascular events, according to the American Heart Association summary on CPAP adherence and recurrent cardiovascular events.
That matters in clinic because many heart failure patients are not just managing dyspnea. They’re managing total cardiovascular risk.
CHF with central sleep apnea and Cheyne-Stokes respiration
This is the group that requires more nuance. These patients may not fit the classic snoring profile. They may describe frequent awakenings, air hunger, insomnia-like sleep fragmentation, or a bed partner may report rhythmic waxing and waning breathing rather than obvious obstruction.
In this phenotype, CPAP may help by stabilizing breathing and improving cardiac mechanics, but only when the pattern is central and the patient is an appropriate candidate. The sleep study matters here. You need the event type, burden, and context, not a vague note that says “sleep apnea present.”
A sleep study report that doesn’t clearly separate obstructive from central events is often not enough to guide heart failure management.
What to look for before referral or initiation
Rather than relying on one symptom, look for a cluster:
- Persistent CHF symptoms despite therapy
Ongoing fatigue, nocturnal dyspnea, or poor functional recovery should raise suspicion. - Nighttime breathing clues
Witnessed apneas, choking episodes, cyclical breathing, or unexplained awakenings matter. - Mismatch between daytime status and symptom burden
If the echo and exam don’t fully explain how poorly the patient feels, nighttime pathology may be contributing. - Sleep study details
Ask for the actual interpretation. “Sleep apnea” is not specific enough.
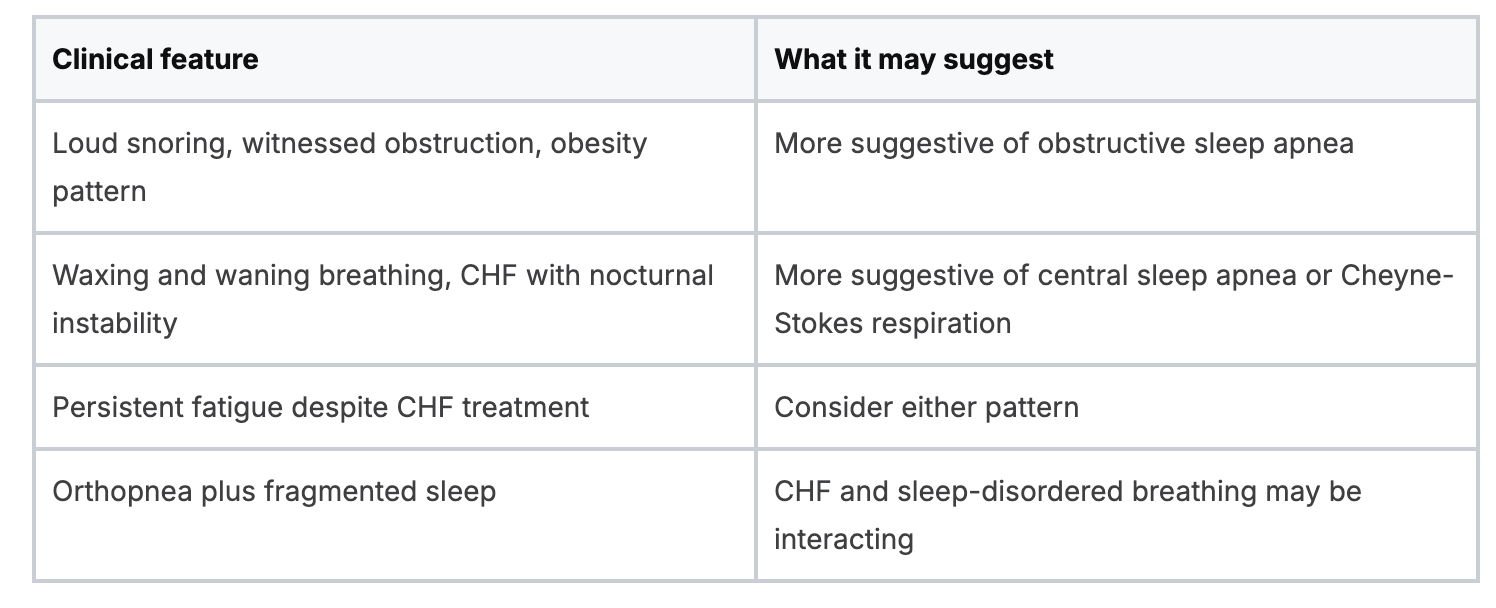
A quick comparison for busy practice
In other words, the best candidates for cpap and chf are not defined by heart failure alone. They’re defined by the interaction between heart failure and the specific form of sleep-disordered breathing present.
Assessing the Benefits and Risks of CPAP
Clinicians do better with CPAP when they discuss it openly. Patients sense very quickly whether we’re describing a realistic treatment or promising a cure-all.
The benefits can be substantial in the right person. The limits are also real. Mask discomfort, pressure intolerance, and poor adherence can derail therapy even when the physiology makes sense.
What goes well when CPAP works
Successful therapy often improves several domains at once. Patients may sleep more continuously, wake with fewer symptoms, and show better day-to-day stability. In carefully selected CHF patients, you may also see improved tolerance of usual heart failure management because the patient is no longer spending every night in repeated respiratory stress.
That doesn’t mean every patient feels dramatically better in a week. Some changes are gradual. The biggest early clues are often less chaotic sleep, fewer nocturnal awakenings, and improved morning function.
Where problems show up
The most common barriers are practical, not theoretical.
- Mask fit issues can lead to leaks, skin irritation, and frustration.
- Pressure discomfort can make exhalation feel awkward, especially for new users.
- Dryness or congestion can reduce willingness to continue.
- Mismatched expectations can make patients quit before adaptation occurs.
There’s also a hemodynamic caution in fragile patients. Positive pressure changes preload and afterload. That can be beneficial, but in a patient with marginal blood pressure or very low-output physiology, aggressive settings may not feel or function well. Those patients need careful monitoring and tighter coordination between cardiology and sleep medicine.
An overlooked enhancer of benefit
Positional strategy deserves more attention than it usually gets. In CHF patients with Cheyne-Stokes respiration, elevating the head of the bed to 45° reduced the apnea-hypopnea index from 34.7 to 23.2 in a study summarized in the JAHA review on position and sleep-disordered breathing in heart failure.
That matters because not every non-responder needs immediate escalation in device complexity. Sometimes position, comfort, and adherence optimization should come first.
Don’t treat CPAP failure as a single event. Ask whether the problem is diagnosis, pressure, mask, sleep position, or patient coaching.
CPAP versus alternatives in the real world
When patients ask about alternatives, it helps to explain that the choice depends on the sleep apnea type. Oral appliances may have a role in selected obstructive cases, but they are not equivalent substitutes for all CHF patients with sleep-disordered breathing.
For clinicians managing airway support more broadly, this review of advanced airway options and best practices is useful when the conversation extends beyond routine outpatient PAP therapy into higher-acuity respiratory management.
Practical Guidance for Managing CPAP in Your Patients
The best CPAP plans are simple enough for patients to follow and specific enough for teams to monitor. In heart failure care, that usually means fewer assumptions and more structured follow-up.
Start with the right patient and the right question
Don’t start with “Does this patient want CPAP?” Start with “What problem are we trying to solve?”
A reasonable workflow looks like this:
- Confirm persistent clinical concern
The patient has ongoing CHF symptoms, suspicious nighttime breathing, or unexplained fatigue. - Define the sleep phenotype
Review the sleep study carefully. Separate obstructive from central events. - Match therapy to physiology
CPAP works best when the diagnosis and mechanism fit the intervention. - Set expectations early
Patients do better when they know adaptation takes coaching and repetition.
What to monitor after initiation
Once therapy starts, follow-up should be more concrete than “How are you doing with the machine?”
Ask about:
- Nightly use pattern
Is the patient using it consistently or abandoning it after the first few hours? - Subjective response
Fewer awakenings, less dyspnea, improved energy, and reduced morning headache all matter. - Cardiovascular tolerance
Check blood pressure trends, volume status, and whether symptoms improve or worsen. - Technical barriers
Mask leaks, dryness, pressure discomfort, and claustrophobia are fixable if you ask directly.
A lot of clinicians already think this way in acute respiratory care. The same structured mindset helps here. If you teach teams the difference between respiratory distress and respiratory failure, they’re usually better prepared to recognize which CHF patients need routine PAP follow-up versus higher-acuity reassessment.
Troubleshooting that actually helps
Patients rarely say, “My issue is poor interface seal and pressure intolerance.” They say, “I can’t do this.”
That complaint usually breaks down into one of a few categories:
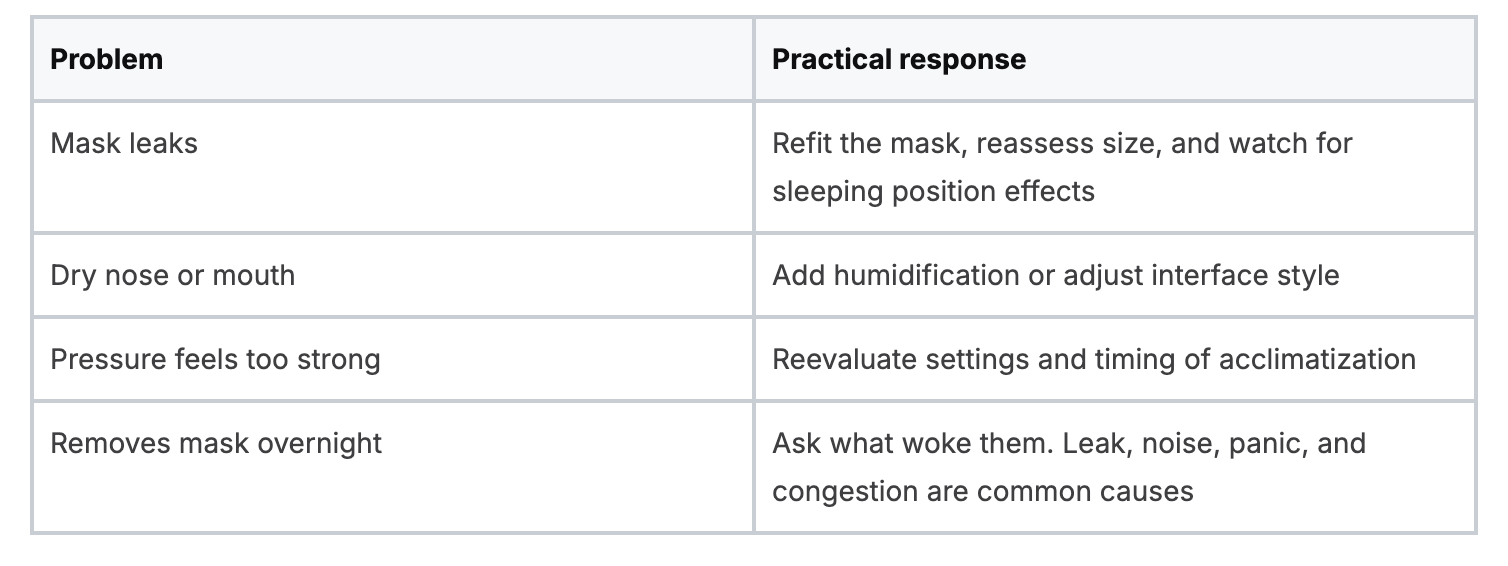
Here’s a brief teaching tool that works well during patient visits:
Why team-based management works better
Heart failure clinicians tend to focus on volume, rhythm, perfusion, and medications. Sleep specialists focus on event type, interface, titration, and adherence. Respiratory therapists often know exactly why a patient is failing the device at home.
Those perspectives are complementary. Patients do best when the team shares the same mental model. The question isn’t whether the problem belongs to cardiology or sleep medicine. It usually belongs to both.
Practice habit: Review CPAP adherence data and CHF symptom trends in the same follow-up window. Looking at one without the other can miss the story.
Staying current without pausing your schedule
This area changes fast enough that many clinicians need refreshers. Online CE and certification are especially useful here because clinicians can revisit pressure concepts, heart failure physiology, and troubleshooting without waiting for an in-person event. That format is not second-tier education. In current practice, it’s often the most realistic way for working professionals to stay current and apply what they learn quickly.
The broader field is moving in that direction. Many hospitals and organizations increasingly accept accredited online education because it meets the needs of modern clinical schedules while preserving quality and accountability. The old belief that only AHA or Red Cross in-person formats are valid doesn’t reflect how healthcare education works today.
Conclusion The Future of Integrated Cardio-Sleep Care
The strongest lesson in cpap and chf is that nighttime physiology matters. A patient can be medically managed by every daytime measure and still lose ground overnight through repeated apnea, oxygen instability, and sympathetic surges.
That’s why integrated care works better than siloed care. When cardiology, sleep medicine, nursing, and respiratory care approach the same patient with a shared framework, CPAP becomes easier to use well. We select better candidates. We interpret sleep studies more carefully. We troubleshoot earlier. We stop calling patients “noncompliant” when the underlying problem is an unaddressed barrier.
The clinical message is straightforward:
- CPAP is most useful when the sleep phenotype is defined clearly
- Obstructive and central patterns should not be managed as if they are the same
- Adherence, mask fit, and sleep position can determine whether a good therapy succeeds
- Heart failure management improves when overnight breathing is treated as part of the disease, not as an unrelated side issue
Education has to evolve with that reality. Clinicians no longer need to rely only on old in-person models to build real competence. Accredited online CE and certifications are now a practical, credible way to master evolving topics, maintain flexibility, and keep skills current. That shift is not lowering standards. It’s matching education to how clinicians actually learn and practice.
It’s also worth saying plainly that AHA and American Red Cross in-person classes are not the only valid path for healthcare professionals. Many recognized online options now provide high-quality, guideline-aligned training that fits real schedules and real clinical demands. The field is moving toward broader acceptance because the format works.
If you care for heart failure patients, this topic belongs in your regular clinical toolkit. Not as an elective interest. As a core part of risk reduction, symptom management, and coordinated chronic care.
If you’re ready to build stronger, more flexible clinical skills through modern online learning, ProMed Certifications offers accredited courses for ACLS, BLS, PALS, CPR, neonatal resuscitation, CE, and CME. Their fully online format is designed for busy healthcare professionals who want credible education without the scheduling limits of in-person classes, and it reflects where healthcare training is headed.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)