

How to Become a Cardiovascular Perfusionist
.png)
You may be reading this from a nursing station, an ICU break room, or your kitchen table after another long shift, thinking the same thing many clinicians think at some point. You want a role with deeper specialization, more technical decision-making, and a direct seat in high-acuity care.
That's where perfusion often enters the conversation.
If you're trying to figure out how to become a cardiovascular perfusionist, the simple checklist is easy to find. The harder part is understanding what the path feels like, why admissions are competitive, and what makes one applicant look ready while another looks interested but untested. That practical layer is what matters.
Is a Career as a Perfusionist Right for You
A perfusionist isn't just the person who runs a machine in the operating room. In cardiac surgery, this professional temporarily manages circulation and oxygenation when the patient's heart is stopped. Think of the role as becoming the patient's heart and lungs for a critical stretch of time.
That's why the job attracts a very specific kind of person. The best-fit candidates usually like physiology, equipment, and real-time problem solving. They also tend to stay calm when the room gets quiet and serious.
A familiar example is the experienced bedside clinician who wants more procedural intensity. A cardiac nurse, respiratory therapist, or surgical team member may start wondering whether they'd rather be at the center of cardiopulmonary support than adjacent to it. If that sounds like you, perfusion may be worth serious consideration. If you're still comparing nursing pathways, this overview of career options for registered nurses can help place perfusion in the broader context.
What the work feels like
Perfusion combines three things that don't often live in one role:
- Deep physiology: You need to understand circulation, oxygenation, temperature management, and how the body responds under surgical stress.
- Technical control: You work with advanced support systems and must understand setup, monitoring, and adjustment.
- Team communication: Surgeons, anesthesiologists, nurses, and perfusionists rely on tight communication during high-stakes moments.
Practical rule: If you want variety every hour, perfusion may feel too narrow. If you want mastery in a narrow, critical domain, it can be a strong fit.
Questions to ask yourself
Before you commit to prerequisites and applications, be honest about your preferences.
- Do you enjoy precision work? Perfusion rewards people who like accuracy more than improvisation.
- Can you tolerate pressure well? The role can involve long procedures and moments where quick judgment matters.
- Are you comfortable with delayed gratification? The training path is specialized, selective, and not fast.
- Do you like being essential without being the public face? Perfusionists are central to outcomes, even if patients may never fully understand the role.
If you read that list and feel energized rather than intimidated, you're probably asking the right career question.
The Foundational Roadmap to Becoming a Perfusionist
The cleanest way to think about this path is as a blueprint. You build the academic base first, add the professional framework, then prove you can apply it in real clinical settings.
A commonly described route is to earn a bachelor's degree, complete a CAAHEP-accredited perfusion program that usually lasts about 2 years, and then qualify for ABCP certification, which brings the total timeline to about six years or more from the start of undergraduate study, according to this overview from Nurse.com on becoming a cardiovascular perfusionist.
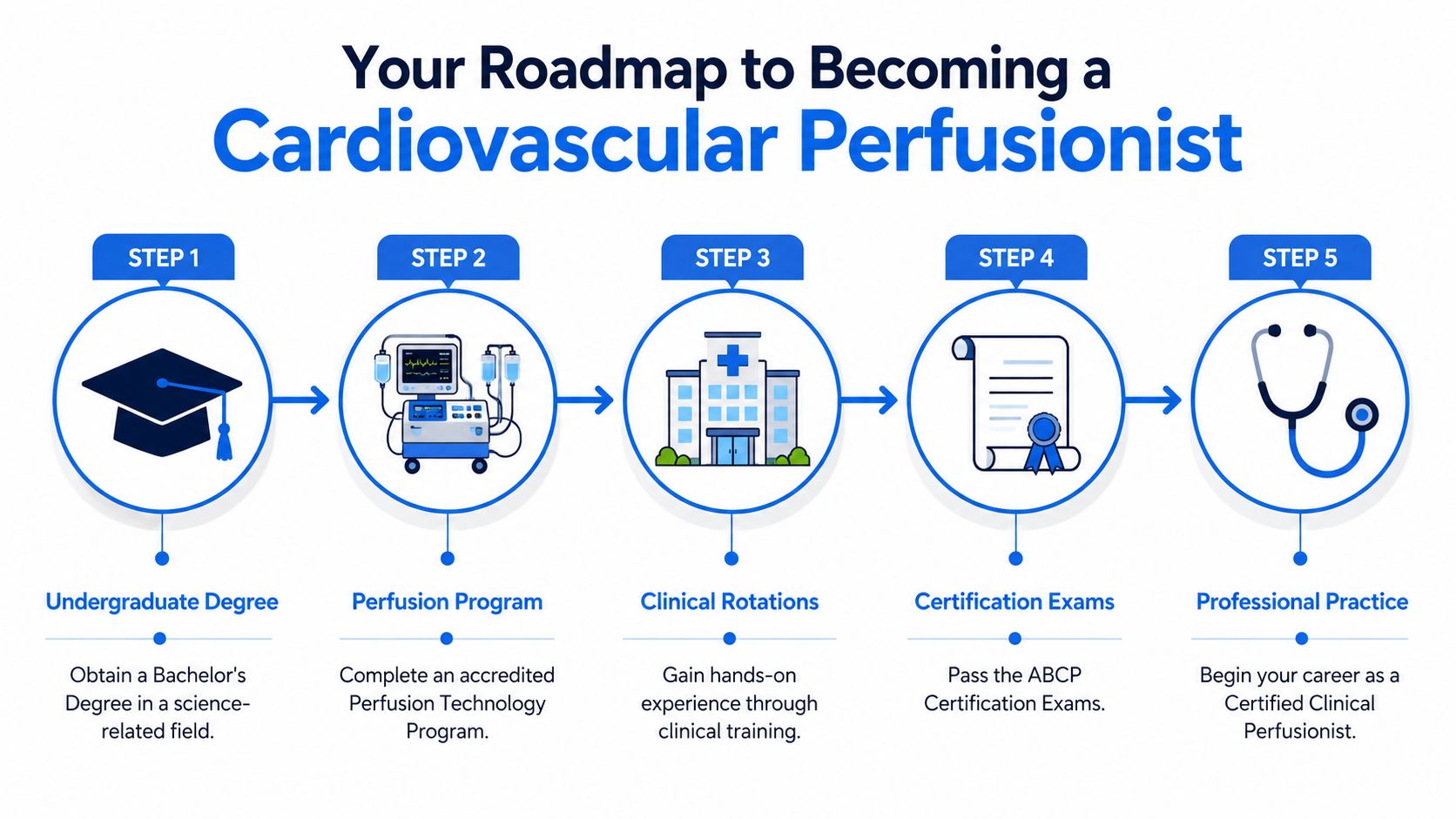
The five major stages
- Earn a bachelor's degree
Most applicants start with a science-heavy undergraduate background or another healthcare-related degree meeting the needed prerequisites. - Complete an accredited perfusion program
This is the specialized training phase where perfusion stops being an idea and becomes a professional discipline. - Finish clinical rotations
You don't become employable by theory alone. Clinical training teaches you how the operating room functions. - Pass certification requirements
Board certification is the professional gate that turns training into recognized practice. - Move into professional practice
After that, your learning continues on the job, especially in cardiac surgery programs and other advanced circulatory support settings.
Why the roadmap matters
Many people underestimate the front end. They think the primary hurdle is perfusion school itself. Often, the bigger challenge is positioning yourself to get in. Program prerequisites, relocation realities, and clinical exposure can make the process feel more like graduate admissions than a simple allied health application.
If you're returning to school or changing direction after time in the workforce, a practical guide for adult learners entering university can help you think through admissions planning, transcripts, and application readiness.
For some applicants, related certifications also help maintain cardiac care familiarity while preparing for the next step. One option is ACLS Certification. ProMed Certifications offers a quick and convenient way to get ACLS-certified, with an online course format that can be completed anywhere and, according to its course information, a card available in as quick as one hour or less after passing the exam.
The roadmap is straightforward on paper. What makes it hard is not confusion about the steps. It's meeting the standard for each step in a small, specialized field.
Your Educational Path and Program Prerequisites
The academic side of perfusion starts long before you enter an operating room. Programs want applicants who can handle advanced physiology, chemistry, and fast clinical reasoning. That's why the undergraduate phase matters so much.
A common pathway is a bachelor's degree followed by an accredited perfusion training program, totaling about 5 to 7 years of preparation. One example highlighted by Perfusion.com's guide to becoming a perfusionist notes programs can run for 22 continuous months and may list tuition of $87,000 for 60 credit hours, which tells you this is a postgraduate clinical track, not a short certificate.
Degrees that usually make sense
There isn't one single perfect major, but some backgrounds line up better with perfusion admissions and training.
- Biology or physiology: Strong fit for students who want a classic science foundation.
- Chemistry: Useful if you're comfortable with rigorous coursework and want a deep scientific base.
- Nursing or respiratory therapy: Often attractive because they combine science with patient care experience.
- Other health sciences: Good options if they include the required prerequisite courses.
The key isn't the title of the degree alone. It's whether your coursework proves that you can handle intense biomedical content.
Courses programs commonly care about
Many applicants get tripped up here because they assume “science degree” is enough. It often isn't. Programs typically look closely at specific prerequisite courses such as:
- Anatomy and physiology: These are central because perfusion depends on understanding organ systems under stress.
- Chemistry: You need comfort with core chemical principles that support blood gas and metabolic concepts.
- Physics: This matters more than many applicants expect because perfusion equipment and flow dynamics are grounded in physical principles.
- Math or quantitative coursework: Programs want evidence that you can work carefully with measurements and calculations.
What makes an application academically strong
Good grades matter, especially in the sciences, but admissions committees usually read for more than transcript quality.
A stronger academic profile often includes:
- Consistent performance: A steady record in foundational sciences usually looks better than scattered excellence.
- Recent readiness: If your earlier academic work is old, newer coursework can show you're still capable of succeeding in a demanding program.
- Clear direction: Your transcript should make sense as a preparation path, not look accidental.
If your GPA is acceptable but your science record is uneven, post-baccalaureate coursework can be more helpful than simply applying and hoping the committee overlooks weak preparation.
Shadowing is not optional in spirit
Even when a program doesn't frame shadowing as an absolute requirement, observation hours can make a major difference. Perfusion is niche. Admissions committees want reassurance that you understand the pace, the environment, and the narrowness of the role.
That matters because applicants often romanticize perfusion. Shadowing forces your interest to become informed.
A smart approach is to keep a brief record of what you observed, what surprised you, and what you learned about the OR team dynamic. Those notes become useful later when you write your personal statement or prepare for interviews.
Mastering Clinical Training and Gaining Experience
Your first weeks in clinical training can feel like standing in an airport control tower while every screen matters at once. Numbers change fast. The room has a clear chain of command. People speak in short, precise language because the patient cannot wait for anyone to get organized.
That pressure is the point of training. Perfusion school teaches the science, but clinical rotations teach timing, judgment, and consistency under supervision. A student may understand cardiopulmonary bypass on paper and still need time to become steady in a live operating room.
Case exposure matters because repetition builds recognition. After enough supervised cases, setup becomes more methodical, pre-bypass checks become less awkward, and changes in the patient's status are easier to spot early. Clinical training turns isolated facts into working habits.
Programs vary, but the progression is usually gradual. Early rotations often focus on watching the room, learning the flow of the case, and understanding how the perfusionist communicates with surgeons, anesthesiologists, and nursing staff. Later, students take on more of the technical work with close oversight.
That progression usually includes experience with:
- Machine and circuit setup
- Safety checks before bypass
- Monitoring pressures, flows, and blood gases
- Responding to cues from the surgical team
- Documenting the case accurately
- Maintaining composure during unexpected changes
The goal is not to memorize a script. The goal is to become dependable in a setting where small errors can become clinical problems very quickly.
This is also where applicants often misread the profession. Getting into perfusion school is competitive, but succeeding once you arrive presents a different challenge. The operating room rewards people who can stay detail-focused for long stretches, accept feedback without defensiveness, and improve steadily from case to case.
Prior clinical experience can help a lot here. Someone coming from respiratory therapy, ICU work, ECMO support, or another acute care role already understands alarms, sterile protocol, documentation pressure, and team hierarchy. That does not make perfusion easy. It does shorten the cultural adjustment.
A useful comparison is learning to drive in a simulator and then merging onto a busy highway. The simulator teaches the controls. Clinical training teaches pacing, anticipation, and calm decision-making when several things happen at once.
If you are still building toward perfusion school, this section has a practical message. Shadowing shows you what the job looks like. Hands-on healthcare experience shows admissions committees that you are more likely to handle the training environment well. In a field with limited program seats, that distinction can strengthen your application in a very real way.
Certification, Salary, and Career Outlook
Certification is the point where perfusion stops being an academic goal and becomes a hiring standard. After training, graduates work toward the credential recognized across the profession: certification through the American Board of Cardiovascular Perfusion, or ABCP.
That matters because hospitals are not hiring for a role that can be learned loosely on the job. They need proof that a candidate has met a defined clinical benchmark and can be trusted in a setting where timing, precision, and judgment all affect patient safety.

What certification means in practical terms
A useful way to understand certification is to compare it to a pilot checkride. Coursework and clinical rotations teach the mechanics. Certification confirms that an outside body accepts your readiness to perform the job at a professional level.
For employers, that translates into two practical signals:
- You met an established professional standard
- You are entering a field with ongoing competency expectations, not a one-time credential
Perfusion is a small profession, and that small size affects both opportunity and competition. The Explore Health Careers perfusionist profile describes a specialized workforce, notes average compensation for experienced certified clinical perfusionists at about $110,000 per year, reports a broader range of roughly $65,000 to $135,000, and explains that only about 18 to 19 perfusion schools operate in the United States.
That last point shapes the career outlook more than many applicants expect.
What the salary picture really means
Perfusion compensation often looks attractive from the outside. The better way to read it is as the result of scarcity, training intensity, certification requirements, call coverage, and the pressure of working in high-acuity surgical care.
Early-career earnings can vary by region, call schedule, case mix, and employer type. A graduate joining a major cardiac center may see a different package than someone working in a smaller hospital system or mobile perfusion setting. Benefits, on-call pay, overtime structure, and relocation support can matter almost as much as the base salary.
That is why salary research should be handled the same way applicants handle admissions research. Look past the headline number and compare the full package, the training support, and the long-term fit. The same discipline used in reviewing competitive application strategies for selective healthcare programs also applies here. Surface-level numbers rarely tell the whole story.
Why job prospects stay favorable
Perfusion does not operate like a broad healthcare career with hundreds of training pipelines feeding the market each year. It works more like a narrow bridge. Few programs train students, certification is required, and hospitals need clinicians who can step into a very specific operating room role.
That creates a pattern worth understanding:
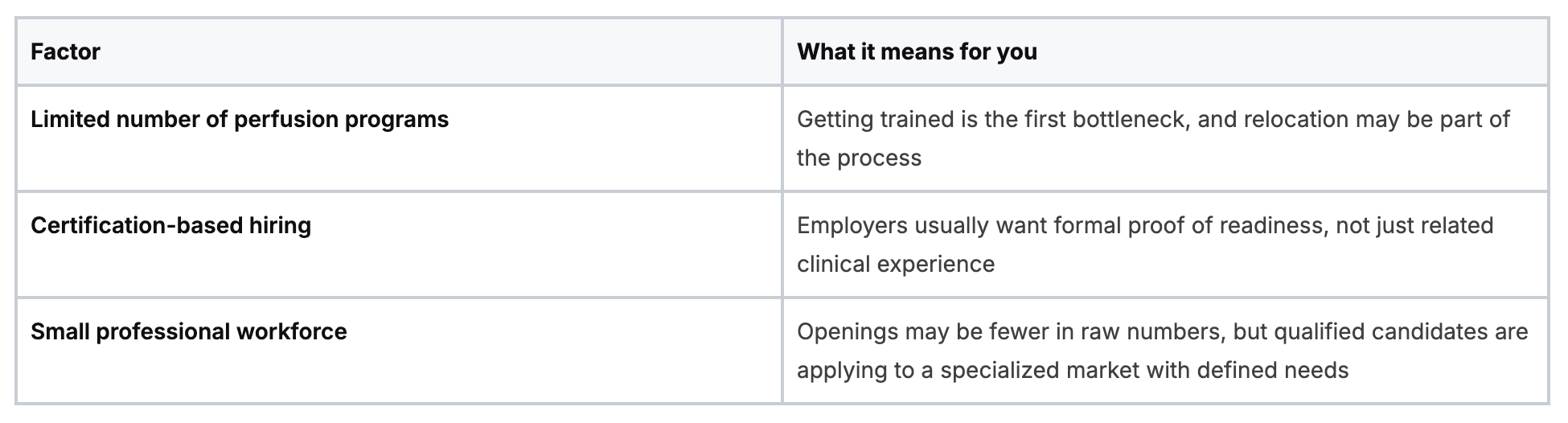
This is one reason the profession can be both promising and hard to enter. Demand exists, but access is filtered early. Students compete for limited seats. Graduates then move into a smaller job market that rewards technical skill, reliability, and willingness to work where openings exist.
How to Build a Competitive Application
Meeting minimum requirements doesn't make you competitive. In perfusion admissions, it often just makes you eligible to be compared with stronger applicants.
A major bottleneck is the limited number of seats across only 18 to 19 schools in the U.S., and many applicants improve their readiness by first working as an ICU nurse or respiratory therapist, as discussed in this article from iPerfusion on becoming a perfusionist in the United States.
What programs are really trying to assess
Admissions committees aren't only asking, “Can this person pass classes?” They're also asking:
- Will this person function well in a high-pressure clinical training environment?
- Do they understand what perfusion is?
- Have they shown commitment to patient care before applying?
- Will they adapt to the narrow, technical nature of the field?
That's why prior healthcare experience can matter so much. An applicant with ICU, respiratory, surgical, or emergency background has already proven something important. They've worked in environments where physiology, urgency, and teamwork are not theoretical.
Moves that make an application stronger
These steps often separate a curious applicant from a convincing one:
- Gain direct patient-care experience: ICU nursing, respiratory therapy, and similar roles can strengthen both your practical readiness and your personal statement.
- Secure shadowing with a certified perfusionist: This shows informed interest, not just career browsing.
- Write specifically in your statement: Describe what you observed, why perfusion fits your strengths, and how your past clinical work prepared you.
- Apply strategically: Don't assume every program has the same prerequisites, residency expectations, or placement realities.
A strong application tells a coherent story. Your academics, experience, and motivation should all point in the same direction.
Borrow strategies from other competitive healthcare admissions
Many of the same habits that help nursing applicants also help future perfusionists. This guide on best practices when submitting nursing school applications is useful because it reinforces practical fundamentals like organization, timely documentation, and presenting a clear professional narrative.
One more point matters here. Don't chase perfusion only because the role sounds advanced. Admissions committees can usually tell when an applicant is drawn mainly to prestige or salary. The strongest candidates sound grounded. They understand the work, the limitations, and the responsibility.
Maintaining Certification with Modern Continuing Education
Perfusion doesn't end at first certification. Like many advanced clinical careers, it requires ongoing learning, updated knowledge, and regular professional maintenance.
That's where some healthcare professionals still get stuck in outdated thinking. Many assume only in-person courses from a short list of organizations count as legitimate continuing education. That isn't how modern healthcare learning works anymore. High-quality online CE and certification formats are a normal part of professional development, especially for clinicians balancing call schedules, long shifts, and family obligations.
Why online learning fits modern clinical practice
Busy professionals need education that works with real life. Online CE gives clinicians more control over pace, location, and timing. For recertification and related credentials, that flexibility can mean the difference between staying current smoothly and constantly scrambling near deadlines.
This is especially relevant for professionals who maintain multiple credentials across emergency, cardiac, pediatric, or resuscitation contexts. If you want a broader look at digital education options, this article on continuing medical education online offers a helpful overview.
What to look for in CE and certification options
Not every course format is equal, but “online” by itself is not a red flag. What matters is whether the education is accredited, current, clinically relevant, and accepted where you work.
Use this checklist:
- Accreditation matters: Verify that the CE or certification provider meets the standards relevant to your profession.
- Guideline alignment matters: The content should reflect current clinical practice, not old algorithms or outdated recommendations.
- Practical access matters: If the course is hard to schedule, many clinicians postpone it longer than they should.
- Employer acceptance matters: Always confirm your workplace or board expectations if you have a specific requirement.
The old assumption that only AHA or American Red Cross in-person classes are valid is too narrow for today's education environment. Many healthcare institutions and professionals now recognize accredited online formats for CE and certifications, especially when those formats are designed for working clinicians.
A realistic approach for working professionals
If your schedule is unpredictable, online education often makes better sense than waiting for a classroom date that may not fit your life. That's not lowering the bar. It's choosing a format that makes completion more realistic and more sustainable.
One example is ProMed Certifications, which offers online medical certification courses for healthcare professionals. Its course catalog includes options such as ACLS, BLS, PALS, CPR, and neonatal resuscitation in a self-paced format designed for busy schedules.
For perfusionists and aspiring perfusionists alike, that kind of flexibility fits the reality of modern healthcare. You still need rigor. You just don't need unnecessary friction.
If you're building your next step in healthcare, ProMed Certifications offers online certification and continuing education options designed for working clinicians who need flexible, current training without putting their schedule on hold.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)
.png)