Home Health Agency Training: 2026 Compliance Guide

You're probably feeling this already. A new hire is ready to start. Your scheduler wants coverage. Your clinical manager wants proof of competency. Your state survey binder is missing a document. And somewhere in the middle, you're trying to answer a basic question that shouldn't be this hard: what should a solid home health agency training program look like?
For many agency owners, training grows in pieces. One checklist from a consultant. One orientation packet from a prior employer. A few shadow shifts. A handful of annual modules. It works until it doesn't. Then a survey, complaint, or documentation review exposes the gaps.
A better approach is to build training like you'd build a care plan. Start with the required baseline. Add the realities of the patient population. Document every step. Reassess often. And make the system workable for real people with real schedules.
The biggest shift I recommend is simple. Put online education at the center of your training model, not on the sidelines. In home care, staff are mobile, schedules change, and competency needs constant reinforcement. An online-first structure gives you control, consistency, and records you can retrieve when someone asks for them.
Your Guide to Modern Home Health Agency Training
A new agency director once described her onboarding process to me like this: “We have good people, but every hire starts differently.” One aide got a thick binder and a hurried orientation. Another shadowed a field clinician for a day. A third completed some videos, but nobody could quickly confirm which ones. Nothing was malicious. The system just grew without a design.
That's common in home care because the work itself is decentralized. Unlike a hospital unit, your staff don't report to one floor with one educator watching the same workflow unfold all day. They travel. They work alone. They enter homes with different family dynamics, layouts, risks, and expectations. So your training system has to do more than teach tasks. It has to create consistency across a scattered workforce.
Think of home health agency training like building guardrails on a winding road. You can't control every turn a caregiver will face in the field. You can control whether they know the rules, can recognize danger, and have a reliable path for getting support.
That's why rigid, classroom-only thinking falls short. It assumes learning only counts if everyone sits in the same room at the same time. In practice, agencies need something far more useful: standardized knowledge delivery, documented completion, flexible scheduling, and clear competency sign-off.
Practical rule: If your training model only works when everyone is physically available at once, it probably won't scale in home care.
The strongest programs use online education for policy review, core knowledge, annual refreshers, and role-based learning. Then they reserve supervisor time for what can't be delegated to a screen: direct observation, coaching, and hands-on validation. That's not cutting corners. That's matching the training method to the skill.
Laying the Foundation for Compliance
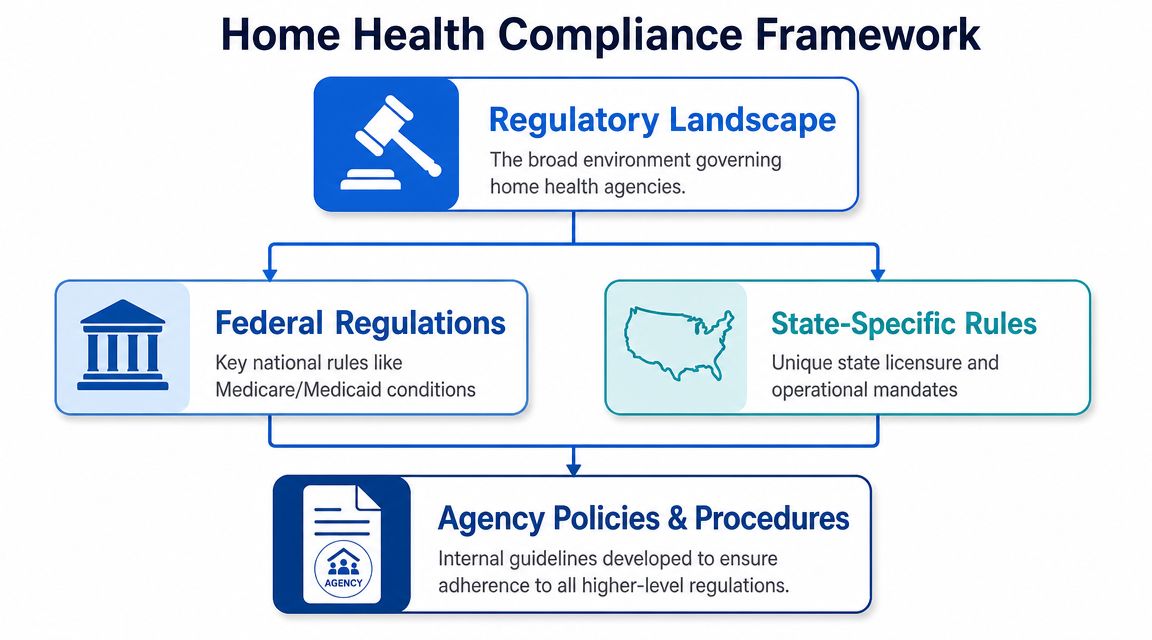
Before you build modules, assign courses, or print a single checklist, you need a compliance map. In home care, training rules come from more than one place. Federal standards may apply. State rules may add more. Then your own agency policies must tie those requirements into daily operations.
Start with the federal floor
For home health aides in Medicare- or Medicaid-certified agencies, federal standards mandate at least 75 hours of training. The same framework requires 16 hours of classroom instruction before 16 hours of supervised practical training, plus competency evaluation and defined subject areas and performance standards.
That federal rule matters because it still shapes the market. The same source notes that 33 states do not require more than the 75-hour federal minimum, while 6 meet the National Academy of Medicine's 120-hour recommendation. That tells you something important. There isn't one neat national model. There is a baseline, then a patchwork.
If you're a new owner, don't make the mistake of treating “federal compliant” as “fully compliant.” Federal rules are the floor. They are not always the ceiling.
Then verify your state-specific obligations
State rules can change the hour count, the pathway, the documentation burden, and the acceptable training format. They may also distinguish between roles that sound similar to a new owner but carry different legal meanings.
Use this quick hierarchy when reviewing your requirements:
- Federal certification rules
If you participate in Medicare or Medicaid, confirm the minimum aide training and competency standards that apply. - State licensure and aide rules
Check whether your state adds training hours, skill validations, exams, approval requirements, or specific instructor standards. - Agency policy requirements
Build internal procedures that are stricter when needed. For example, your agency may require extra documentation practice before field release.
Training compliance fails most often at the handoff between these levels. The law says one thing, the policy says another, and the manager in the field is improvising a third version.
Build your document trail early
Most compliance problems aren't caused by a total lack of training. They're caused by poor proof. An aide may have finished orientation, but can you show the assigned content, completion date, competency result, and supervisor sign-off in one place?
That's why agencies should tie training design to records management from day one. A good system to streamline healthcare document workflows helps you keep orientation records, policy acknowledgments, competency forms, and in-service logs organized before they become a survey problem.
A simple working rule helps here: if a regulator asked for the record tomorrow, could your team produce it without searching five inboxes and two filing cabinets?
What compliance should cover in practice
Your training foundation should clearly account for:
- Required subject matter such as the core topics your governing rules expect aides to learn.
- Competency evaluation so you can distinguish knowledge exposure from demonstrated ability.
- Role-specific application because aides, nurses, supervisors, and office staff don't need identical training.
- Documentation retention so completion isn't just remembered. It's retrievable.
Compliance isn't glamorous. But it's the frame that holds everything else up. If that frame is weak, even good teaching won't protect the agency.
Designing Your Core Training Curriculum
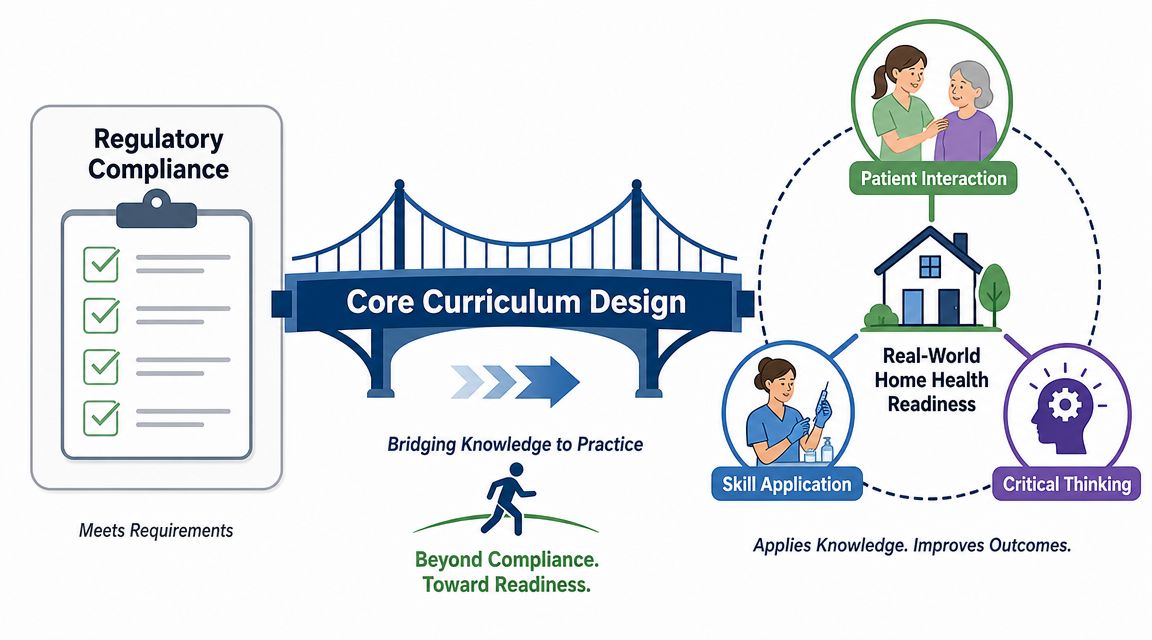
A compliant curriculum checks the required boxes. A useful curriculum prepares staff for what happens in the home. Those aren't always the same thing.
One of the most helpful findings I share with agency leaders comes from a needs assessment of home health providers. It identified five recurring training difficulty categories: medical device usage, patient and family education, family involvement, provider isolation, and communication barriers.
Teach for the home, not the classroom
Many agencies often drift off course by building a curriculum around topics instead of situations. Staff sit through infection control, HIPAA, patient rights, and documentation modules, but still feel unsteady when a family member challenges instructions, a device alarm sounds, or they can't reach a supervisor quickly.
A stronger curriculum organizes training around field realities.
Consider how that looks in practice:
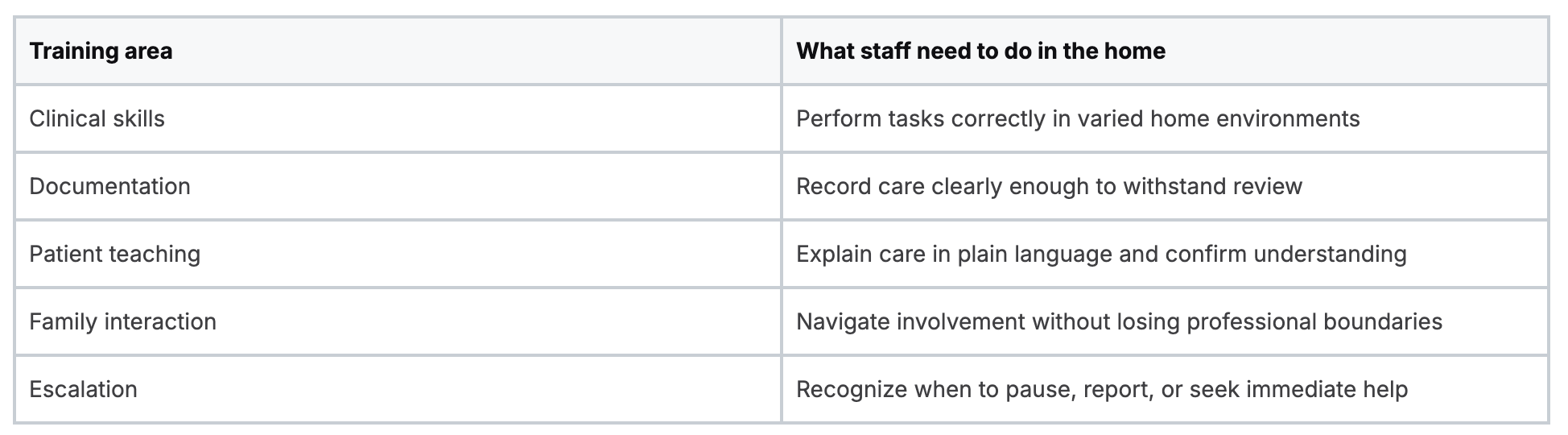
That structure changes the conversation from “Did they complete the module?” to “Can they perform safely under pressure?”
Use scenarios to close common gaps
Scenario-based training works especially well in home care because the work is contextual. The same blood pressure reading means different things depending on the patient, the plan of care, and what else the aide sees in the home.
Build scenarios around the gaps agencies repeatedly encounter:
- Device handling: A patient has equipment in the home and the caregiver must identify what looks normal, what doesn't, and when to escalate.
- Teach-back with families: An aide explains a care step, then confirms the patient or caregiver can repeat it back in their own words.
- Boundary setting: A family member asks the caregiver to perform something outside the care plan.
- Working alone: The caregiver notices a change in condition and must follow the agency's reporting path without immediate in-person backup.
- Documentation under scrutiny: The caregiver completes a note that matches what was observed and done.
Good curriculum design treats communication as a clinical safety skill, not a soft extra.
Separate knowledge from readiness
Course completion and job readiness aren't the same. A staff member may understand a concept on a quiz and still struggle to apply it in a cluttered home with an anxious caregiver nearby.
That's why your curriculum should have two layers:
- Knowledge layer through online modules, readings, short assessments, and policy review
- Performance layer through observation, return demonstration, coaching, and sign-off
When agencies combine those layers well, staff arrive in the field with more than memorized rules. They arrive with a playbook.
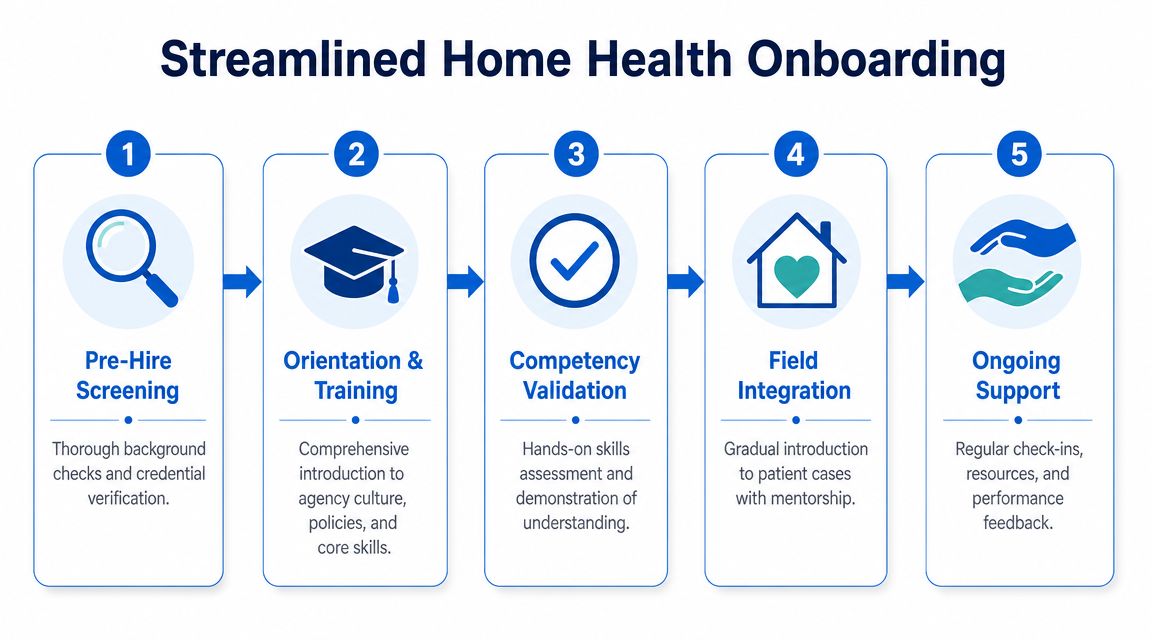
Building an Effective Onboarding Workflow
Onboarding is where your agency's values become visible. If the process is disorganized, new hires assume daily operations will be too. If the process is clear, paced, and well documented, they start with confidence.
The most practical benchmark for home health aide training is a blended one. A practical model combines at least 120 hours of classroom or online instruction with 40–60 hours of supervised clinical practice. That same source notes that modern programs often use online coursework for didactic content while reserving in-person time for hands-on skills validation.
The old onboarding model wastes clinical time
Many agencies still use a patchwork method. A new hire comes in for a long first day, signs forms, watches presentations, asks rushed questions, and then waits for someone to schedule skills review. Supervisors repeat the same orientation speech over and over. Paper packets pile up. Important items get missed because everyone is trying to move quickly.
That model creates two problems.
First, it uses high-value clinical educator time for information that could have been delivered more consistently online. Second, it buries the part that needs human observation: competency.
A better workflow is online first and hands-on where it counts
An efficient onboarding flow usually works best in this order:
- Pre-hire verification
Confirm credentials, background requirements, and any role-specific prerequisites. - Self-paced orientation modules
Assign online content for core policies, infection control, privacy, safety expectations, and agency workflows. - Focused live review
Use educator time to answer questions, discuss field judgment, and clarify agency-specific standards. - Hands-on validation
Observe skills, documentation habits, and escalation decisions before field release. - Supported field integration
Pair the new hire with structured follow-up, not silent independence.
That sequence protects staff from overload. It also protects your supervisors from spending their day reading policy slides that a learning platform can deliver more reliably.
Later in the onboarding journey, a brief field support refresher can help managers develop stronger preceptors. This practical guide on being a mentor to newcomers to the healthcare profession is useful for shaping that support role.
Online learning is valid for what it does best
A persistent myth still shows up in healthcare training conversations: that learning only “counts” if it happens face-to-face, and sometimes only through legacy in-person providers. That thinking is outdated.
For knowledge-based content, online education is a strong fit for home care because it offers consistency, repeatability, flexible scheduling, and automatic documentation. Staff can review material when they are alert, revisit difficult topics, and complete required content without commuting to a classroom after a long shift.
The smart position isn't “online for everything” or “in person for everything.” It's method matching. Use online learning for foundational instruction. Use live supervision for observed skills and judgment.
If you can explain why each step happens in the order it does, your onboarding is probably designed well. If the order exists only because “that's how we've always done it,” redesign it.
Managing Continuing Education and Annual Compliance
The hardest training task for many home care agencies isn't initial orientation. It's the ongoing cycle that follows. Staff are dispersed, turnover disrupts schedules, and annual requirements keep arriving whether your calendar is calm or chaotic.
CMS requires at least 12 hours of in-service training each year for certified home health aides. This means agencies must assign, schedule, document, and verify recurring education across a moving workforce.
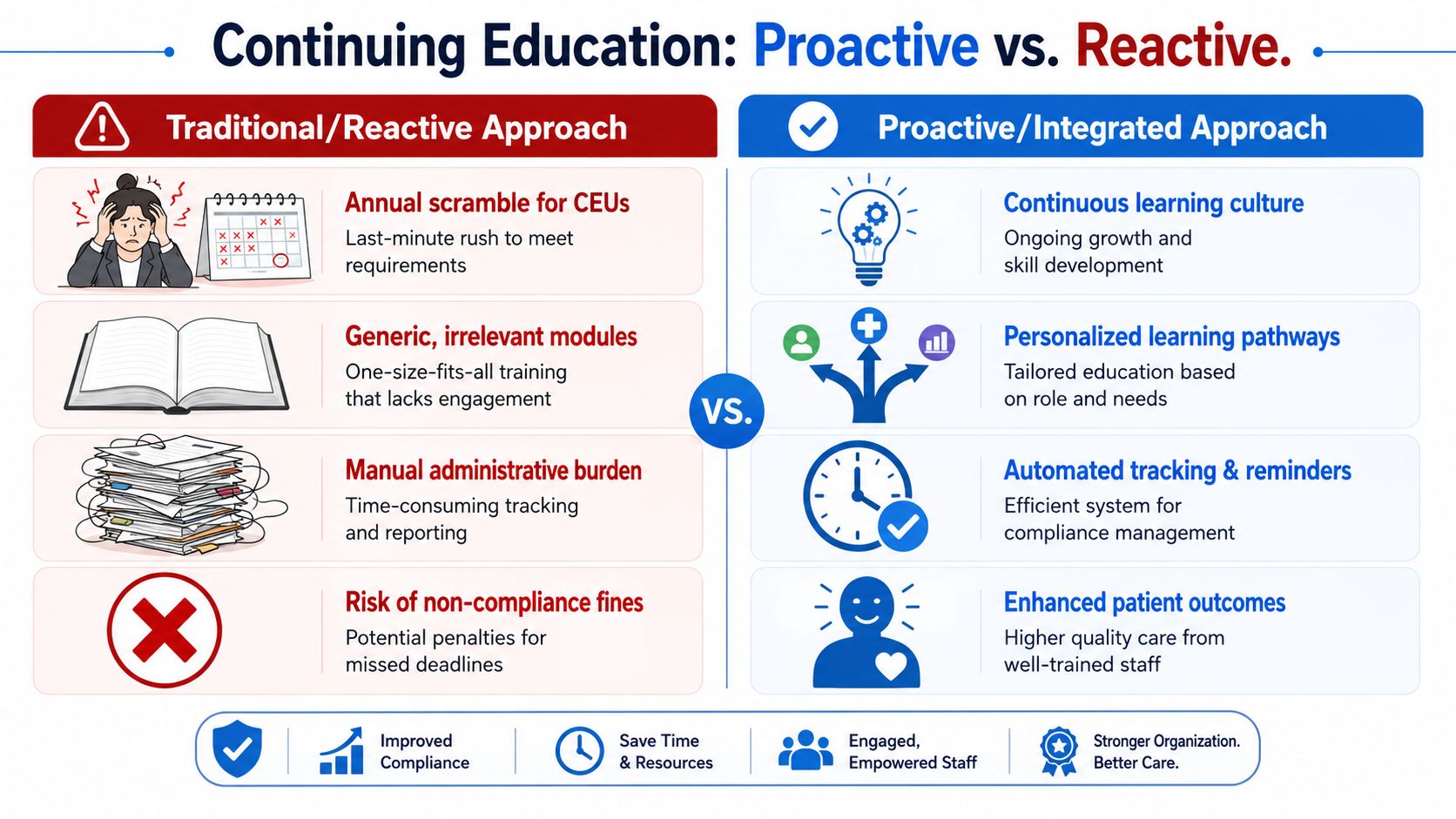
The reactive model creates avoidable risk
You've probably seen the traditional pattern. A deadline approaches. Someone runs a spreadsheet. Managers start emailing reminders. Staff scramble to find time. Certificates arrive in mixed formats. One person completed a module but never submitted proof. Another attended a session but the sign-in sheet is missing.
That system doesn't just drain office time. It makes compliance fragile.
Here's the side-by-side reality:

Why online continuing education fits home care
Home care is one of the clearest examples of where online education makes operational sense. Your workforce doesn't sit in one building. Your educators can't gather everyone easily. Your compliance team needs records fast.
An online platform helps you:
- Assign by role: Aides, nurses, and supervisors can receive different content based on actual responsibility.
- Track automatically: Completion dates, certificates, and overdue items stay visible.
- Reduce off-the-floor disruption: Staff can complete didactic learning without a group classroom event.
- Standardize quality: Every learner receives the same core material, not a shortened version based on who happened to teach that day.
This is also where agencies should challenge another stale assumption: that only AHA or American Red Cross in-person classes are valid options for healthcare professionals. That isn't true as a blanket rule. Acceptance depends on the employer, the credential requirement, and whether the course aligns with needed standards. Many healthcare organizations now recognize accredited online education and certification pathways because they solve real operational problems without sacrificing educational quality.
For leaders juggling broader licensure obligations across clinical roles, this breakdown of continuing education requirements for nurses by state can also help when your home care team includes licensed nursing staff with separate CE demands.
Annual compliance works best when it stops being an event and becomes part of routine operations.
What to require from your CE system
Don't settle for a platform that only hosts videos. Your continuing education system should help you answer practical questions fast:
- Who is overdue right now?
- Which assignments are role-specific?
- Can I produce completion records during a survey?
- Can managers see status without requesting a custom report?
- Can staff complete training without losing an entire workday?
If the answer to those questions is no, the system isn't supporting compliance. It's just storing content.
Auditing Reporting and Improving Your Program
A home health agency training program isn't complete until you can prove it worked. That proof matters during surveys, internal reviews, corrective action plans, and ordinary management decisions.
California is a good reminder of how structured this can get. In that state, a CNA can qualify as a home health aide through a 40-hour state-approved program, while a non-CNA generally needs a 120-hour state-approved program, and both pathways include an exam. The lesson for agency owners is broader than California. States often expect formal milestones and documented proof, not informal assurance that someone was “trained.”
Keep an audit-ready record set
Your files should show the full training story for each worker. At minimum, keep a clean record of:
- Initial training completion with dates and assigned content
- Competency validation with observer name, method, and result
- Annual in-service records with current status
- Policy acknowledgments for required agency procedures
- Corrective or remedial training when performance issues arise
This doesn't have to live in disconnected folders. A centralized compliance system makes retrieval much easier, especially when leadership needs a real-time view across the organization. Agencies reviewing platform options may find this overview of integrated tools that simplify medical compliance helpful as they rethink fragmented tracking methods.
Review trends, not just completions
A smart audit process looks beyond whether people finished modules. It asks where patterns are forming.
If several new hires struggle with documentation sign-off, your orientation content may be clear but your practical examples may be weak. If field staff repeatedly need remediation on escalation procedures, the issue may be workflow design, not motivation. If one branch falls behind on annual training every cycle, the bottleneck may sit with scheduling or manager follow-up.
Survey readiness starts months before a survey. It shows up in whether your records are current on an ordinary Tuesday.
Use training data to improve the program
The best agencies treat training records like quality data. They look for recurring weak spots, update content, and revise supervision methods. They don't wait for a deficiency to tell them what the staff didn't absorb.
That's the standard worth aiming for. Build the program, document the work, review the evidence, and adjust. Home health agency training should be a managed system, not a pile of completed forms.
A strong training program makes compliance easier, onboarding smoother, and continuing education far less disruptive. If you want a flexible online option for healthcare certifications and continuing education, ProMed Certifications offers self-paced courses, group management tools, and organization-friendly workflows built for modern healthcare teams.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)