Glasgow Coma Scale: A Clinician's Essential Guide
.png)
You're in the trauma bay. EMS rolls in a patient after a crash. The room gets loud fast. Someone is placing monitors, someone is asking for vitals, and someone turns to you and asks, “What's the GCS?”
That question matters because the Glasgow Coma Scale gives the team a shared, fast way to describe neurologic status. It turns a vague impression like “he looks out of it” into something more useful and repeatable. If you're new to bedside assessment, it can feel awkward at first. The good news is that once you understand the pattern behind it, GCS becomes one of the most practical tools in your assessment routine.
Assessing Consciousness in Critical Moments
A lot of new clinicians first meet the Glasgow Coma Scale during a stressful moment. A patient arrives after a fall, a head strike, or a possible overdose. You need to know, quickly, whether the patient is awake, confused, following commands, or not responding at all.
That's where GCS helps. It gives you a structured way to assess consciousness under pressure, using observations you can make at the bedside in seconds. It also helps you communicate clearly to the next clinician, the receiving unit, or the provider making treatment decisions.
If you've ever done a rapid neuro check during a broader head-to-toe assessment, you've already used the mindset behind GCS. You're not trying to write a full neurologic consult. You're trying to answer a focused clinical question. How responsive is this patient right now?
Why this tool matters in real life
GCS is useful because it keeps you from relying on loose descriptions.
Instead of saying:
- “He's kind of sleepy” you can describe whether he opens his eyes to voice or only to painful stimulation.
- “She's not making sense” you can describe whether she is confused, speaking in words, or making sounds only.
- “He moved a little” you can describe whether he obeys commands, withdraws, or localizes pain.
Practical rule: In an urgent setting, a simple, structured description is better than a dramatic but vague one.
Many learners get nervous because they think GCS is about memorizing a chart. It isn't. It's really about watching what the patient does and translating that response into a common clinical language. Once you see it that way, the scale gets much easier to use.
Breaking Down the Glasgow Coma Scale
The Glasgow Coma Scale is a standardized method for assessing consciousness and brain injury. It was developed in 1974 by Graham Teasdale and Bryan Jennett at the University of Glasgow, and it replaced more subjective bedside descriptions with a more consistent framework.
It works by scoring 3 components:
- Eye opening
- Verbal response
- Motor response
Those component scores add up to a total score ranging from 3 to 15.
Think of GCS as a shared language
A helpful way to think about GCS is this. It's a universal shorthand for consciousness. One clinician says “E3 V4 M6,” and another clinician immediately understands what the patient did during the exam.
That matters because consciousness is easy to describe poorly. One nurse may say “drowsy.” Another may say “lethargic.” Another may write “arousable.” Those terms can be useful, but they aren't always precise enough on their own. GCS gives the team something more standardized.
Why these three parts
Each component tells you something different.
- Eye opening reflects arousal.
- Verbal response reflects awareness and communication.
- Motor response reflects the patient's ability to follow commands or react purposefully.
Together, they give you a quick snapshot of neurologic function without requiring advanced equipment.
The strength of the scale is its simplicity. It's quick enough for emergency use, but structured enough to track change over time.
This is one reason GCS shows up so often in trauma, emergency, and critical care training. In practice, you'll see it repeatedly in resuscitation scenarios and neurologic assessments. If you're reviewing this skill as part of ACLS Certification, an online format can work well because the scoring logic is highly structured and easy to revisit on your own schedule.
The total score matters, but the parts matter too
New learners often focus only on the final number. That's understandable, but it can hide important detail.
A patient with one total score may look very different from another patient with the same total. That's why experienced clinicians don't just ask, “What's the GCS?” They often want the components too.
Write the exam as components first, then total it. That habit builds accuracy and makes your documentation more useful.
A Step-by-Step Guide to GCS Scoring
GCS scoring is straightforward once you break it into its three parts. Eye opening is scored from 1 to 4, verbal response from 1 to 5, and motor response from 1 to 6. A commonly cited analysis found that the total score predicted acute mortality with 88% accuracy using all three subscales.
Start with what you can observe immediately
Before you touch the patient, watch.
Are the eyes already open? Is the patient speaking? Are they moving purposefully? That first glance often gives you part of the score before formal testing even begins.
Then assess each category in order.
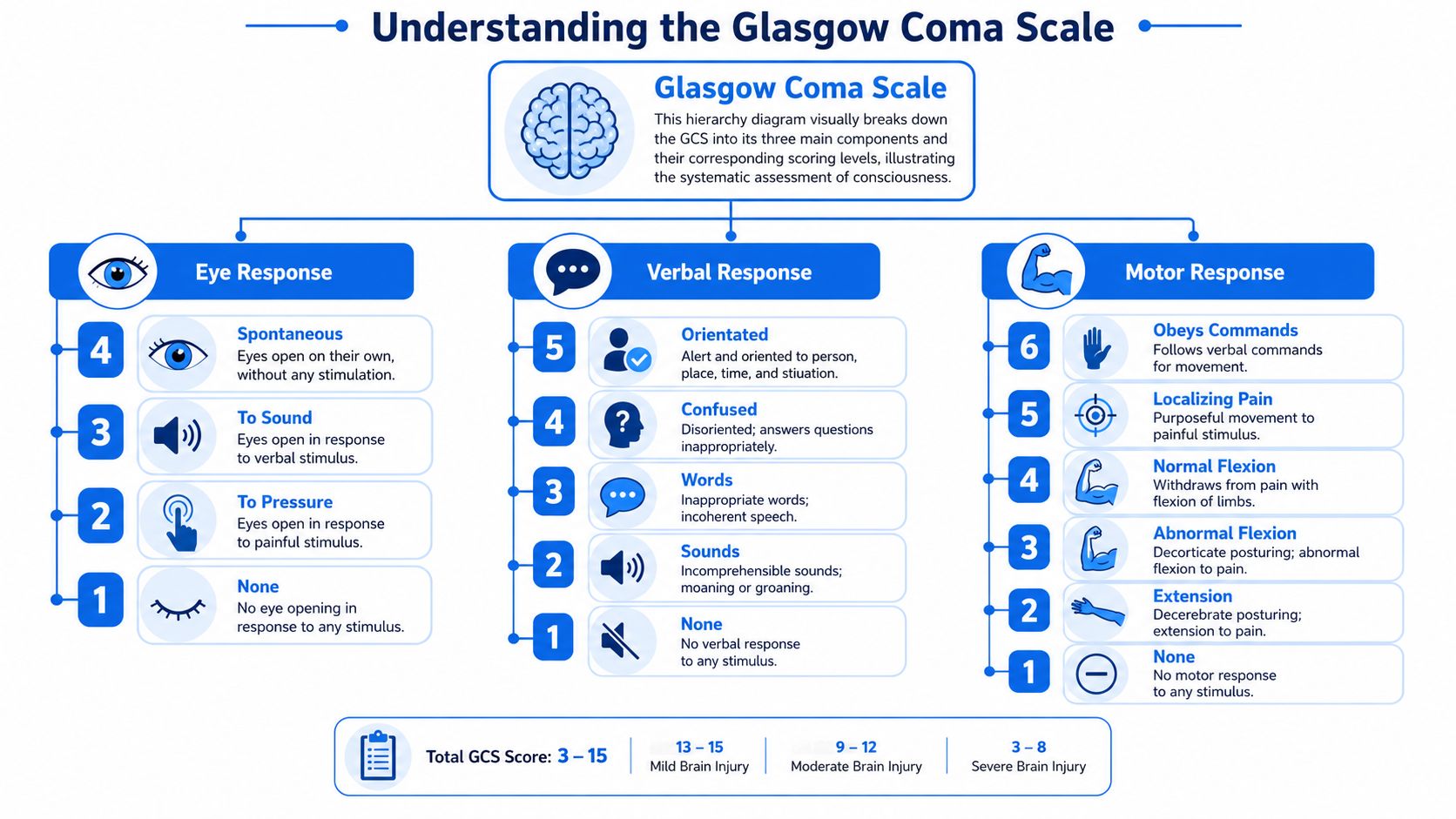
Glasgow Coma Scale scoring chart

How to score eye opening
Eye opening tells you about arousal.
- E4 Spontaneous means the patient's eyes are already open without prompting.
- E3 To sound means the patient opens eyes when you speak or call their name.
- E2 To pressure means the eyes open only after painful stimulation.
- E1 None means no eye opening at all.
Don't overthink this category. Just document the best observed response.
How to score verbal response
Many learners hesitate, especially when responses are messy.
- V5 Orientated means the patient answers appropriately and appears aware of self or situation.
- V4 Confused means the patient is talking but disoriented.
- V3 Words means recognizable words are present, but conversation isn't coherent.
- V2 Sounds means moans or incomprehensible vocalization only.
- V1 None means no verbal response.
A patient doesn't need perfect conversation to earn points here. Listen for the highest level they demonstrate.
How to score motor response
Motor scoring often carries the most weight clinically because it shows whether the patient can act with purpose.
- M6 Obeys commands means the patient follows a simple request such as “squeeze my hand” or “lift your arm.”
- M5 Localizing pain means the patient reaches toward the source of painful stimulation in a purposeful way.
- M4 Normal flexion means withdrawal from pain, but not purposeful localization.
- M3 Abnormal flexion means a flexor posturing response.
- M2 Extension means extensor posturing.
- M1 None means no motor response.
If you're struggling to tell localizing from withdrawing, ask yourself this. Did the patient try to remove or reach toward the stimulus, or did the limb simply pull away?
That distinction takes practice. Bedside repetition helps more than memorization. Resources on patient assessment for paramedics can reinforce this kind of observation-based scoring because the same rapid assessment habits apply across emergency care.
One rule that prevents many mistakes
Always score the patient's best response.
If one arm follows commands and the other doesn't, you score the best motor response observed. The same principle applies across the scale. That keeps the score consistent and avoids underestimating function.
If you're practicing pediatric emergency scenarios, this kind of repeatable framework is one reason many clinicians use online review before exams such as PALS Certification, where you can revisit neurologic assessment details whenever your schedule allows.
Putting GCS Scoring into Practice with Examples
Clinical examples make the scale stick. When you attach the numbers to real bedside behavior, the chart stops feeling abstract.
Example one with a confused trauma patient
A patient arrives after a motor vehicle collision. His eyes are open before you speak to him. He answers questions, but he keeps saying the wrong month and doesn't remember the crash. When asked to squeeze your hands, he does it right away.
That gives you:
- Eye opening E4 because eyes are spontaneous
- Verbal response V4 because speech is present but confused
- Motor response M6 because he obeys commands
Total: GCS 14
This is a classic early example for new learners because it shows that a patient can be awake and talking but still not be fully orientated.
Example two with limited speech after a neurologic event
A patient with suspected stroke opens her eyes when you speak. She cannot produce meaningful speech, but she does make sounds. When you ask her to lift her arm, she follows the command with the unaffected side.
That gives you:
- E3 because eyes open to sound
- V2 because she produces sounds only
- M6 because she obeys commands
Total: GCS 11
A common misinterpretation occurs. People sometimes assume low verbal performance always means globally depressed consciousness. It doesn't. Aphasia can lower the verbal score without reflecting the same overall neurologic picture as diffuse unresponsiveness.
Document what you observe, then think clinically about why the score looks that way.
Example three with an unresponsive overdose patient
A patient is found unresponsive. Eyes stay closed. There is no speech. With painful stimulation, the patient pulls the arm away but does not reach toward the stimulus.
That gives you:
- E1 for no eye opening
- V1 for no verbal response
- M4 for withdrawal from pain
Total: GCS 6
That score signals severe impairment, but the bedside question doesn't stop at the number. You still need to consider airway, breathing, circulation, likely cause, and reversible factors.
How to document these clearly
Good documentation is short and specific.
Instead of writing only a total score, write the components first:
- E4 V4 M6 = GCS 14
- E3 V2 M6 = GCS 11
- E1 V1 M4 = GCS 6
That format tells the next clinician far more than the total alone. It also makes repeat assessments easier. If the score changes later, your team can see which part changed.
Interpreting Scores and Common Clinical Challenges
In routine clinical interpretation, 13 to 15 generally indicates mild injury, 9 to 12 moderate injury, and 3 to 8 severe injury or coma, as outlined in this clinical overview of the Glasgow Coma Scale.
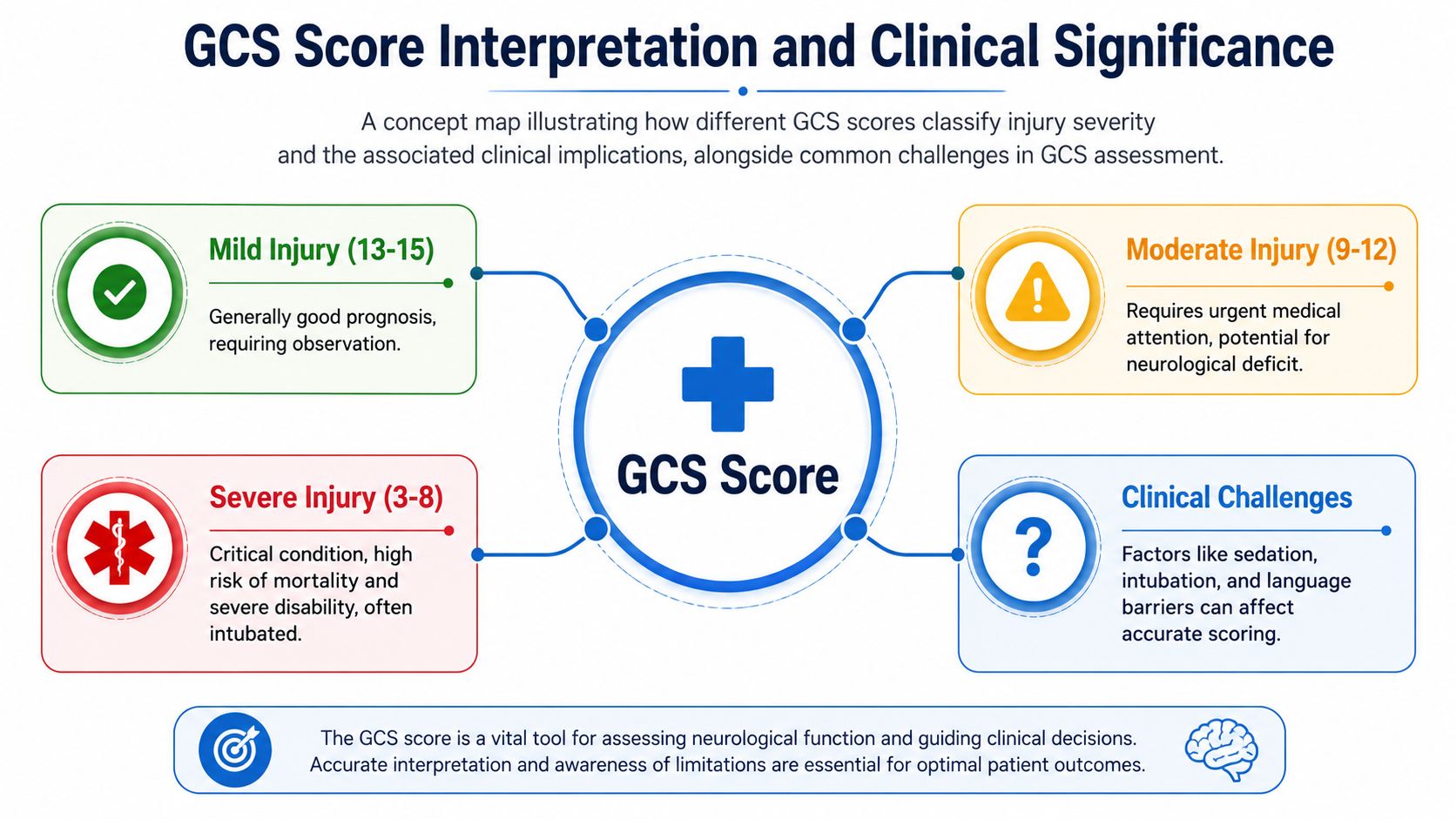
Those ranges are useful. They help teams sort urgency and communicate severity quickly. But they don't tell the whole story.
Why a single number can mislead you
A common phrase in training is that a GCS of 8 means coma or automatically means intubation. That shortcut is memorable, but bedside care is more nuanced than that.
Two patients can share the same total score for very different reasons. One may be sedated. Another may be aphasic. Another may be intubated and unable to produce a verbal response at all. If you look only at the total, you can miss the context that explains the exam.
What to do with untestable components
Modern GCS practice pays close attention to whether the exam is fully testable. Official guidance emphasizes identifying interfering factors such as intubation, sedation, aphasia, facial injury, or neuromuscular blockade, and it supports documenting component scores and modifiers, including approaches such as GCS-P for pupil reactivity, as described by the official Glasgow Coma Scale guidance.
That matters because the raw total can become misleading when a component is artificially suppressed.
For example:
- Intubated patient means verbal response can't be tested in the usual way
- Facial trauma or swelling may block eye opening
- Paralysis or heavy sedation may suppress motor findings
- Language disorder can reduce verbal scoring without the same implication as reduced consciousness
A careful GCS exam doesn't ignore these limits. It names them.
Many clinicians document the component pattern and note the modifier, such as an intubated patient recorded with a notation like 7T alongside the component description. The exact local documentation style may vary, but the principle is the same. Preserve the reason the score is limited.
Trends matter more than slogans
A single GCS is a moment in time. Serial exams are often more helpful.
If a patient drops from obeying commands to withdrawing only, that change matters. If an intubated patient's eye and motor scores improve even though the verbal component remains untestable, that matters too. The scale is strongest when used as a repeated bedside measure, not as a stand-alone rule.
If you teach or review cognitive and neurologic screening broadly, it can help to compare how different tools are scored and interpreted. For example, this guide on mastering MoCA test scoring is useful because it shows the same broader principle. A score is only meaningful when you understand what the patient could and could not reasonably demonstrate during the exam.
For post-resuscitation patients, interpretation gets even more complex because sedation, targeted temperature strategies, and evolving neurologic findings can all affect responsiveness. That's why broader context from post-cardiac arrest care is so important when you're using GCS after return of spontaneous circulation.
Why GCS Mastery Matters for Your Medical Certification
If you work in emergency care, critical care, transport, pediatrics, or inpatient nursing, GCS isn't optional knowledge. It shows up in patient handoff, charting, simulation, and certification prep because it's part of the language clinicians use every day.
The good news is that this is a skill that translates well to online learning. GCS has a defined structure, observable criteria, and repeated clinical patterns. That makes it well suited to digital review, case-based practice, and self-paced repetition. For CE and certification prep, online education can be just as effective as in-person training because learners can pause, replay, and revisit difficult concepts instead of trying to absorb everything in one live session.
Why the format matters for busy clinicians
Healthcare professionals rarely have the luxury of ideal schedules. Night shift, rotating weekends, and family responsibilities make fixed classroom sessions hard to manage.
That's one reason online certification and CE keep gaining acceptance. The old idea that only in-person classes through a few large organizations are valid doesn't match how many clinicians learn today. Hospitals and individual professionals increasingly use accredited online options because they're flexible and practical.
What this means for skill retention
For a tool like GCS, repetition matters more than seat time. You get better by seeing examples, scoring cases, and checking your reasoning. Online review supports that process well because you can return to the exact point where you got stuck.
That's also why many clinicians prefer digital certification prep over a one-day classroom format. When the content is structured and clinically focused, online learning supports confidence, retention, and real-world use.
A practical option is ProMed Certifications, which offers online medical certification courses for healthcare professionals. For clinicians preparing for ACLS, PALS, BLS, CPR, or related recertification, that format gives a way to review core assessment skills like GCS on a schedule that fits actual clinical life.
If you want to strengthen neurologic assessment skills while completing required training, ProMed Certifications offers a fully online path for medical certifications and continuing education. It's a practical option for busy clinicians who need flexible study time without giving up structured, clinically relevant review.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)