

A Guide to Evidence Based Practice in Healthcare
You're probably making evidence based practice decisions already, even if you don't call them that.
A patient asks whether a standard protocol is really the right fit for them. A coworker says, “We've always done it this way.” Your unit adopts a new workflow, and now everyone has to decide whether it improves care or just adds another checkbox. Those moments are where evidence based practice stops being a classroom phrase and becomes daily clinical judgment.
Used well, it helps you make cleaner decisions, explain your reasoning, and adapt care without drifting into habit-based medicine. It also raises an uncomfortable but necessary question. If we expect patient care to follow evidence, shouldn't our own continuing education and certification choices follow evidence too?
What Is Evidence Based Practice?
You are at the bedside, the protocol says one thing, the patient in front of you needs nuance, and a colleague is still relying on a method they learned years ago. That tension is exactly why evidence based practice matters. It gives clinicians a disciplined way to choose care that is current, defensible, and suited to the person in front of them.
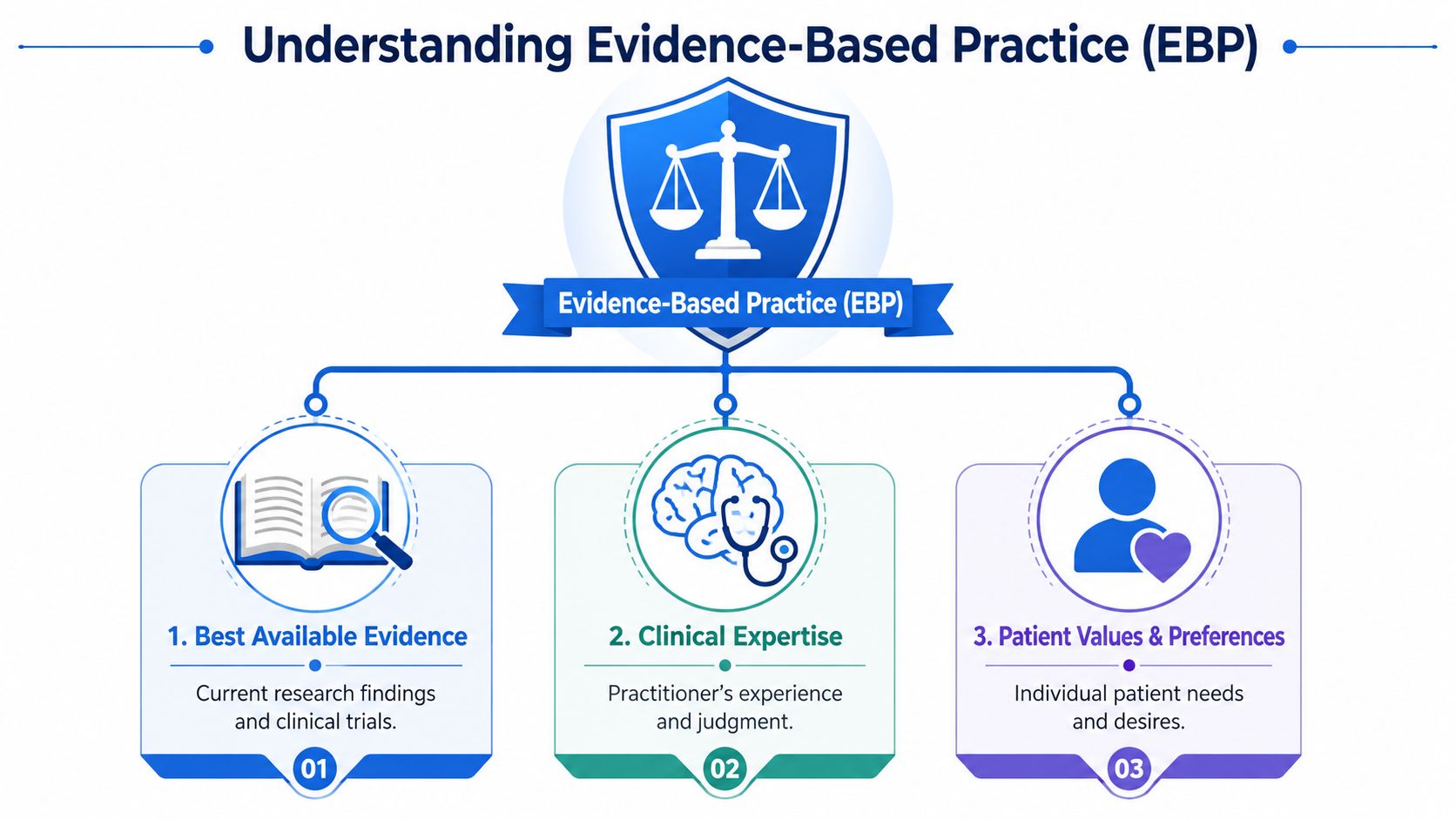
At its core, evidence based practice, or EBP, brings together three inputs: the best available research, clinical expertise, and patient values and preferences. The Agency for Healthcare Research and Quality describes EBP as care informed by the best available evidence while accounting for patient needs and clinician judgment (AHRQ overview of evidence-based practice). If one part is ignored, decision-making gets weaker.
A useful comparison is a three-legged stool. Research gives you direction. Clinical expertise gives you balance. Patient preferences tell you whether the plan can work in real life.
The three parts that hold EBP up
- Best available evidence means current, relevant research that answers the clinical question in front of you.
- Clinical expertise means your ability to judge what is realistic, safe, urgent, and appropriate in a specific setting.
- Patient values and preferences mean the patient's goals, concerns, culture, and daily reality shape the final plan.
New clinicians sometimes get confused here. They hear “evidence based” and assume research outranks everything else. It does not. A treatment supported in the literature still has to fit the patient's condition, risks, preferences, and ability to follow through. In the same way, experience matters, but experience alone can harden into habit if it is never tested against newer evidence.
That same standard should apply to professional education. If healthcare professionals are expected to use evidence instead of tradition at the bedside, we should also question training models built around seat time, travel, and rigid classroom schedules merely because that is how certification used to be done. Evidence supported online learning has made it possible to study, review, and demonstrate competence in ways that better match how adults learn and how clinicians truly work.
EBP is more than reading studies
EBP is not a journal club skill. It is a decision method.
A clinician using EBP does more than locate an article. They form a focused question, look for strong evidence, judge its quality, apply it to a real patient, and then check whether the result was useful in that setting. That last step matters because an intervention that looks good on paper can still fail if it does not fit the workflow, staffing, or patient population.
A simple non-hospital example helps. If someone asks about skin cleansing, the right answer depends on the product, the reason for use, skin sensitivity, and whether ordinary soap would do the job. That is why practical guides like when to use Dial soap are helpful. Good decisions depend on context, not blanket recommendations.
Why this definition matters
EBP protects patients from two common errors. One is habit-based care, where a method survives because no one has challenged it. The other is trend-based care, where a new idea spreads before anyone asks whether the evidence is solid.
It also gives healthcare professionals a better standard for choosing how they maintain competence. A course should not be treated as better because it happens in a classroom or follows an older certification routine. If flexible, evidence-supported online education improves access, supports retention, and fits the realities of clinical practice, then choosing it is not the easy option. It is the evidence based option.
The 5 Steps of the EBP Process
A new nurse finishes a hectic shift, then hears this in report: “We've always taught discharge instructions this way.” That sentence should make any clinician pause. Habit is not a method. The EBP process gives you a method you can use when time is short and patient outcomes are critical.
I teach the five steps as a clinical investigation. You start with a problem, gather the right information, test whether it is trustworthy, use it with judgment, and then check what happened. The sequence matters, much like running a code. If you skip steps, you increase the chance of making a confident decision on weak footing.
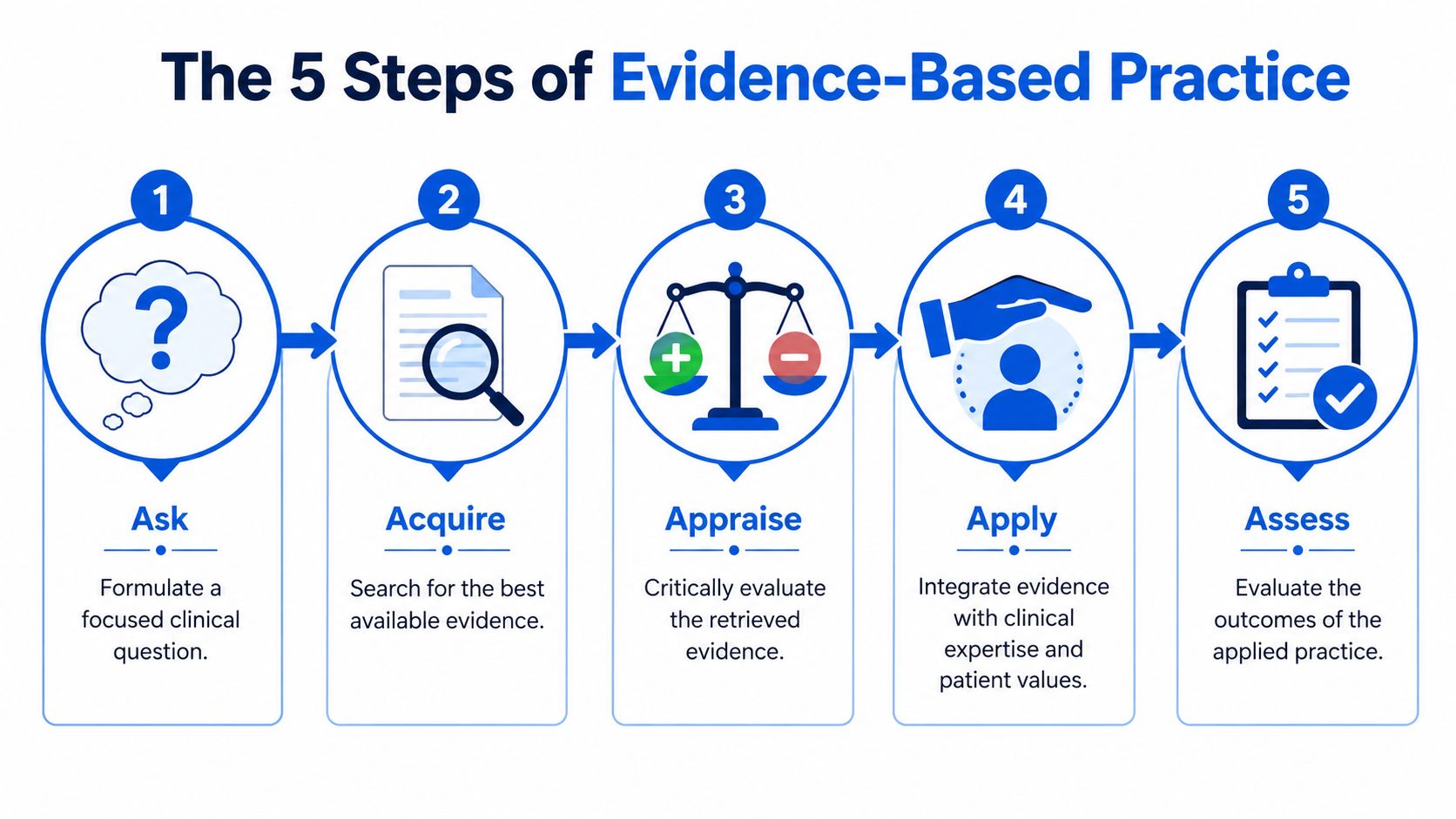
Ask
Start by turning a messy clinical concern into a clear question.
New clinicians often ask broad questions because broad questions feel practical. In reality, they slow you down. “What's the best way to manage this?” could send you in ten directions. A focused question points you toward useful evidence faster.
That level of precision saves time later.
Acquire
Once the question is clear, look for the strongest evidence you can reasonably get.
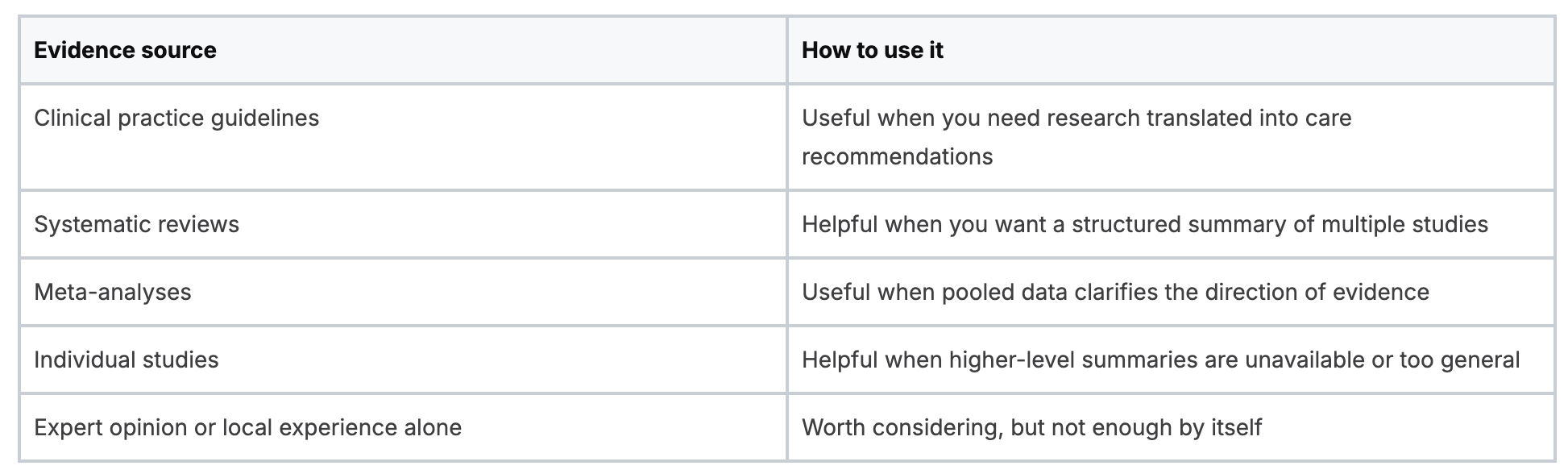
A quick search is not the same as an effective search. Start high in the evidence hierarchy. Guidelines, systematic reviews, and meta-analyses usually give you a better starting point than a single study because they synthesize a larger body of research.
A practical way to sort sources is this:
Evidence sourceHow to use itClinical practice guidelinesUseful when you need research translated into care recommendationsSystematic reviewsHelpful when you want a structured summary of multiple studiesMeta-analysesUseful when pooled data clarifies the direction of evidenceIndividual studiesHelpful when higher-level summaries are unavailable or too generalExpert opinion or local experience aloneWorth considering, but not enough by itself
This search step also applies to professional education. If we say healthcare decisions should follow evidence, our training choices should follow evidence too. A rigid classroom requirement should not win by tradition alone. If an online ACLS or BLS course is well designed, accessible, and supports retention for working clinicians, EBP supports considering that format seriously. For clinicians reviewing current response pathways, this guide to important ACLS algorithms you need to know is a useful example of targeted learning tied to real clinical decisions.
Appraise
Now ask a harder question. Is this evidence good enough, and does it fit your setting?
This is the point where many learners get uncomfortable because appraisal sounds academic. It is a bedside skill. You are judging whether the source is credible, whether the methods are sound, and whether the findings match the kind of patients you serve. A strong paper from a highly controlled setting may still have limited value if your patient population, staffing pattern, or follow-up resources are very different.
Keep the appraisal practical. Was the recommendation developed carefully? Are the results relevant to this patient or unit? Do the findings align with what other high-quality sources report?
That is clinical judgment, not academic decoration.
Apply
Application is where evidence meets the individual patient in front of you.
You combine research evidence with clinical expertise and patient preferences. If a recommendation is technically sound but unrealistic for a patient with low literacy, limited transportation, or competing priorities at home, you adapt. Good care is evidence-informed and person-specific.
The same principle belongs in continuing education. Training should fit how clinicians learn and work. Flexible online education is not a lesser option merely because it breaks from older routines. In many cases, it is a better match for adult learning, shift work, and rapid access to updated content.
Assess
The final step is follow-through.
After you apply the evidence, look at the outcome. Did the patient understand the discharge plan? Did adherence improve? Did the workflow become safer or more realistic for staff? If the answer is no, return to the question, the search, or the appraisal and correct the process.
This step is what keeps EBP honest. It also separates modern education from checkbox education. A course should not count as successful because someone sat in a room or passed a one-time test. It should help clinicians perform better in practice. That is the standard EBP demands.
EBP in Action with ACLS and BLS Examples
Evidence based practice becomes much easier to respect once you see it inside the protocols you already use.
ACLS and BLS aren't built to preserve tradition. They evolve because clinicians, educators, and guideline developers review research, weigh applicability, and refine care standards over time. In other words, the resuscitation training you rely on is one of the clearest everyday examples of evidence based practice at work.

Protocols don't become standards by accident
When a team updates a resuscitation workflow, that change should reflect a careful review of evidence, not a preference for novelty.
That's why strong clinicians don't memorize algorithms as if they dropped from the sky. They ask better questions. What problem is this step solving? What patient outcome is it meant to improve? What signs tell us the protocol fits this patient right now?
What EBP looks like during training
Say you're teaching a new nurse why a sequence matters during a code response. The old habit is to say, “Learn it because that's the rule.”
The better approach is to say:
- This step exists for a reason
- That reason comes from reviewed evidence
- Your job is to understand both the protocol and the patient in front of you
That mindset changes how people learn. They stop treating certification as a memorization exercise and start treating it as clinical preparation.
Here's another example. First aid and emergency response training often works best when people connect protocol to practical safety habits outside the classroom.
The strongest training doesn't just tell clinicians what to do. It helps them understand why the action is recommended and when judgment still matters.
Why this matters for confidence
A clinician who understands evidence based practice usually handles change better.
When guidelines shift, they're less likely to react with frustration or skepticism alone. They recognize that healthcare is supposed to update when evidence improves. That doesn't make every update easy, but it does make the change easier to evaluate and teach.
This is especially important in ACLS, BLS, and similar credentialing environments. If your training culture treats protocols as static doctrine, you end up with compliant learners who may struggle when conditions vary. If your culture treats protocols as evidence-informed tools, you build clinicians who can think, adapt, and explain their care.
Common Barriers to EBP and How to Overcome Them
Most clinicians don't resist evidence based practice because they dislike science. They resist it because real healthcare settings are crowded with time pressure, staffing gaps, uneven training, and institutional habits that are hard to move.
I've seen this play out in familiar ways. A unit wants to improve care but nobody has time to search and appraise evidence during a busy shift. A manager supports EBP in theory but defaults to whatever the department has always accepted. A clinician works with patients whose barriers make a polished guideline harder to apply than it looked on paper.
The barrier isn't always knowledge
A major challenge is the gap between EBP as a clinical ideal and EBP as a workforce implementation problem. A 2024 review emphasizes that underserved communities face intersecting barriers tied to race, socioeconomic status, and geography, and those barriers shape how evidence can be used in practice. The same review also aligns with the broader concern that EBP often needs local adaptation rather than universal application.
That matters more than many training programs admit.
A guideline may be sound, but if your patient population faces transportation issues, language barriers, housing instability, or low trust in the healthcare system, implementation can break down quickly. In those moments, the question isn't whether EBP failed. The question is whether the team confused published evidence with usable practice.
Four barriers I see most often
- Time pressure
Clinicians often think EBP requires hours in a database. In reality, a focused question and a smart search strategy save more time than repeated trial-and-error care. - Access problems
Some teams have limited access to journals, librarian support, or protected review time. That makes appraisal harder, especially for early-career staff. - Cultural resistance
“We've always done it this way” still has too much power in healthcare. Tradition can be useful, but it isn't a substitute for appraisal. - Rigid views of training
One overlooked barrier is the belief that only certain in-person classes from familiar brands count as legitimate learning. That mindset slows adoption of more flexible education models, even when those models align well with current evidence, adult learning needs, and workforce realities.
If an organization says it values evidence but dismisses modern education formats without reviewing their quality, that organization has an EBP problem.
How to respond without burning out
You don't need to become the unit's full-time researcher to support evidence based practice. You do need a repeatable approach.
Try this:
- Start with one recurring problem
Pick a question your team faces often. Frequent problems create the clearest payoff. - Use shared appraisal criteria
Agree on how your group will judge quality and fit. That reduces opinion battles. - Adapt for local reality
A recommendation may need changes for staffing, language access, or follow-up limits. - Measure something after adoption
Even a simple outcome check is better than assuming success. - Treat education as part of implementation
If staff can't access training in a realistic format, practice change will stall.
This last point deserves more attention than it gets. Many EBP efforts fail because education delivery is treated as an afterthought instead of part of the implementation plan.
The Modern Way to Fulfill Your CE and Certification Needs
A night-shift nurse finishes a 12-hour stretch, checks an expiring certification, and sees the usual obstacle course ahead. Rearranging shifts, driving to a classroom, sitting through fixed lecture blocks, and hoping the schedule works with family responsibilities. If we would reject a care plan built on convenience and tradition alone, we should question an education model chosen for the same reasons.
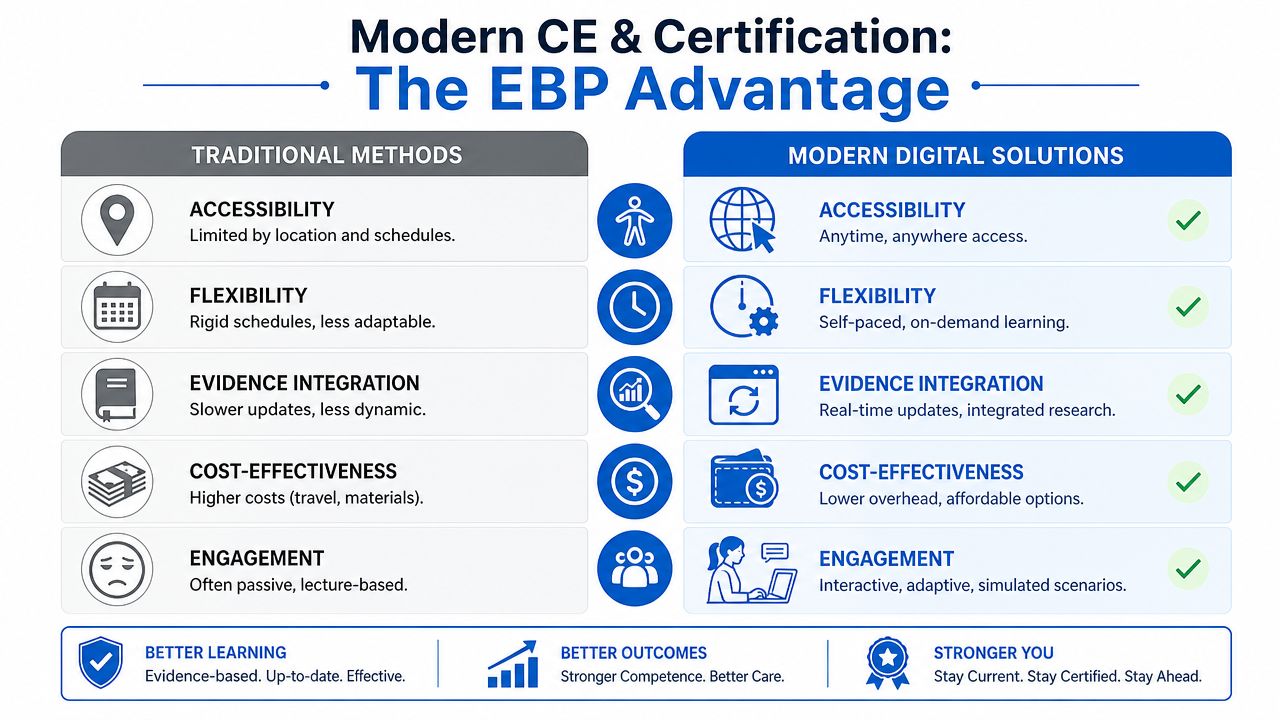
The old assumption is simple: if people sit in the same room, learning must be better. Clinical educators know it is not that simple. Good learning depends on whether the content is current, the design supports retention, the format allows review, and the learner can complete the training without disrupting patient care or personal responsibilities.
That matters more than many organizations admit. A clinician who can revisit rhythm recognition, medication steps, or algorithm changes after a course has an advantage over someone who had one live exposure and no practical way to review. Education works like skill maintenance in practice. Repetition, access, and timely refreshers shape performance.
Digital delivery also fits the operational reality of healthcare. Rotating shifts, staffing shortages, travel time, childcare needs, and multi-site teams all affect whether required education gets done well or gets done late.
A practical comparison

The point is not that every online course is strong. The point is that format alone does not determine quality.
Evidence based practice asks clinicians to judge methods by the strength of support behind them, not by habit or brand familiarity. That standard should apply to continuing education too. If an online course is accredited, aligned with current guidelines, instructionally sound, and accepted by the relevant employer or board, dismissing it because it is not classroom-based is weak reasoning.
Many training policies fall behind modern care. Healthcare systems ask clinicians to adapt quickly, stay current, and document competency, yet some still treat inflexible delivery models as the default mark of seriousness. That approach confuses tradition with rigor. Rigor comes from standards, assessment, and relevance to practice.
For a closer look at how digital formats support ongoing professional development, see this article on continuing medical education online. ProMed Certifications is one example of an online provider offering medical certification courses for healthcare professionals in areas such as ACLS, BLS, PALS, CPR, and neonatal training.
If education is part of implementation, then choosing an accessible, evidence-supported learning format is part of evidence based practice too.
Embrace the Future of Healthcare Education
Evidence based practice is more than a clinical method. It's a professional mindset.
It asks you to combine strong evidence, informed judgment, and the needs of the person in front of you. It also asks you to work through a disciplined process. Ask, acquire, appraise, apply, and assess. When you use that habit consistently, you make better decisions and you become more adaptable when healthcare changes.
That same mindset belongs in continuing education and certification. If a learning format is accessible, current, accredited, and built for how clinicians practice, it deserves serious consideration. Clinging to outdated assumptions about what “counts” doesn't strengthen standards. It often blocks them.
If you're rethinking how you learn, this overview of the basics of eLearning for online medical certification is a strong place to start. The future of healthcare education isn't about abandoning quality. It's about delivering quality in formats that professionals can use consistently, responsibly, and well.
If you're ready to align your learning with the same evidence-based mindset you bring to patient care, explore ProMed Certifications. Their online certification and continuing education options give healthcare professionals a flexible way to stay current, meet requirements, and keep learning without unnecessary scheduling barriers.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)
.png)