

A Guide to the Pulseless Electrical Activity Strip in ACLS

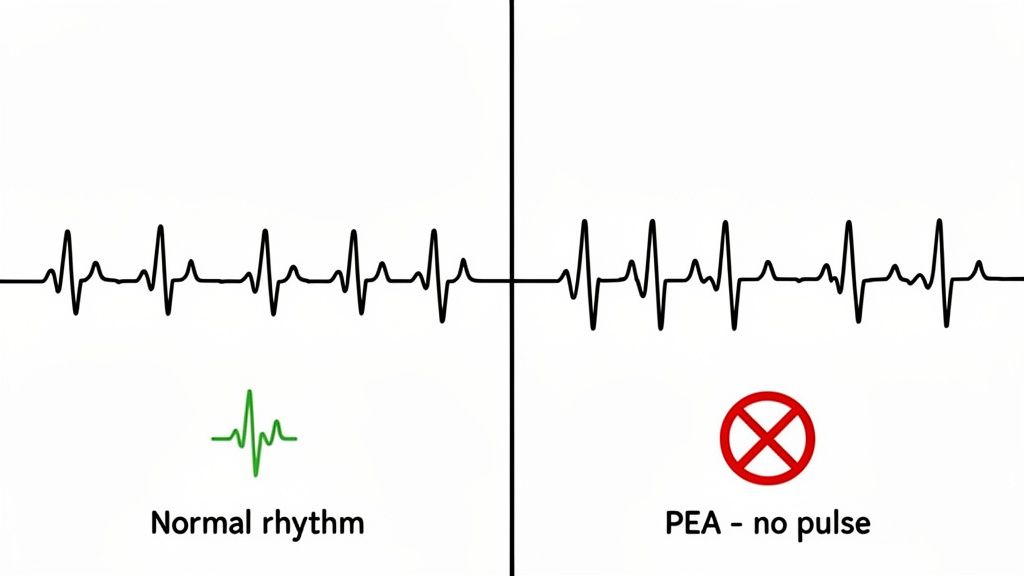
When you're in the middle of a code, few things are as unnerving as a pulseless electrical activity (PEA) strip. The monitor shows an organized rhythm, sometimes one that looks almost normal, but when you reach for a carotid or femoral pulse, you feel nothing.
It’s like looking under the hood of a car to find the engine humming perfectly, yet the wheels refuse to turn. This is PEA: a complete and catastrophic disconnect between the heart's electrical signals and its mechanical ability to pump. This is electromechanical dissociation, and it’s a true emergency. This guide will help you confidently identify a pulseless electrical activity strip and master the ACLS protocol for it.
What a Pulseless Electrical Activity Strip Reveals
Unlike the flatline of asystole or the chaotic scribble of ventricular fibrillation, a PEA strip can be incredibly deceptive. The heart's electrical conduction system is still firing away, dutifully creating what look like P waves, QRS complexes, and T waves. The "instructions" for a heartbeat are being sent.
The problem is, the heart muscle isn't listening. It’s failing to contract with enough force to actually move blood through the body. Your first and most important job is to recognize this dangerous paradox: organized electrical activity on the screen, but a lifeless patient in the bed.
To put PEA in context, it's helpful to see how it stacks up against the other major cardiac arrest rhythms you'll encounter.
How PEA Compares to Other Cardiac Arrest Rhythms
| Rhythm | ECG Activity | Palpable Pulse | Initial ACLS Action |
|---|---|---|---|
| PEA | Organized rhythm (not VF/VT) | No | CPR and Epinephrine |
| Asystole | Flatline (no electrical activity) | No | CPR and Epinephrine |
| VF/pVT | Disorganized or very fast, wide rhythm | No | Defibrillation |
| Normal Sinus | Organized, normal rate rhythm | Yes | Monitor (not in arrest) |
This table makes the distinction clear: PEA and asystole are the two non-shockable rhythms. When you see one of these, grabbing the defibrillator paddles won't help. The immediate focus must shift to high-quality CPR and figuring out why the heart stopped pumping.
Why This Rhythm Is So Critical
Identifying a PEA strip is a skill every provider must have, because it immediately changes your course of action. Since it's a non-shockable rhythm, the ACLS protocol instantly pivots to two priorities:
- Starting high-quality CPR to do the work the heart can't.
- Running through the reversible causes—the H's and T's—to find and fix the underlying problem.
The stakes are incredibly high. Survival from PEA is notoriously poor. Globally, survival to hospital discharge for PEA is only around 4–7%, a stark contrast to the 17–21% for shockable rhythms. In the U.S., data shows a similar trend, with PEA survival at about 8% compared to over 30% for VT/VF. You can explore the research on PEA survival rates to dig deeper into these outcomes.
Think of it like this: The ECG shows that the heart's "blueprints" for a heartbeat are being sent, but the "construction crew"—the heart muscle—isn't building anything. Your job is to figure out why the crew stopped working.
Grasping this is fundamental to earning your ACLS, PALS, or BLS certification. The outdated belief that only stuffy, in-person classes could provide valid training is fading fast. Study after study has shown that high-quality, accredited online education delivers results that are just as good, if not better, in terms of knowledge retention and convenience.
As more hospitals and healthcare systems embrace these modern online options, you can get the critical training you need on your own time. ProMed is at the forefront of this shift, offering fully accredited, AHA-aligned courses that give today's healthcare professionals the flexibility and credibility they require.
Why PEA Is More Common Than Ever in Cardiac Arrest
If you’ve been in medicine for a while, you've probably noticed a major shift in the cardiac arrests you respond to. For years, the textbook cardiac arrest was Ventricular Fibrillation (VF)—that chaotic, shockable rhythm. But the reality on the ground today looks very different.
Pulseless Electrical Activity (PEA) has steadily climbed the ranks to become one of the most common initial rhythms we see. This isn't just a bit of medical trivia; it's a fundamental change that directly impacts how we run a code. Understanding why PEA is so much more prevalent is the first step to mastering it.
The Shifting Landscape of Cardiac Arrest
The data tells a compelling story. Back in the 1980s, VF was the star of the show, kicking off 61–65% of out-of-hospital cardiac arrests (OHCA). PEA was a much smaller piece of the pie. Fast forward to today, and those numbers have practically flipped.
Recent studies show that PEA now accounts for 22–30% of arrests in many areas, while VF has taken a backseat. You can read the full research on this significant trend in cardiac arrest rhythms to dig into the data yourself. So, what’s behind this dramatic change? It boils down to a few key factors that are, ironically, signs of medical progress.
Widespread Medication Use: Modern pharmacology is a double-edged sword. Medications like beta-blockers and other antiarrhythmics are incredibly effective at preventing or stopping shockable rhythms like VF. The catch? They stabilize the heart's electrical system but do nothing for the underlying mechanical problem, which can leave you with an organized rhythm but no pulse—the very definition of PEA.
Implanted Defibrillators (ICDs): More patients than ever have an ICD, which acts like a tiny, internal paramedic. It shocks them out of VF or VT the moment it happens. This is a lifesaver, but it means that by the time you arrive, the patient has already been defibrillated. The shockable rhythm is gone, and what's often left is PEA or asystole.
Improved Public CPR: With faster bystander response and better quality CPR, it's more common for VF to be converted into an organized rhythm before EMS even gets there. But if the root cause of the arrest isn't fixed, that organized rhythm won't generate a pulse, and you're left managing a PEA arrest.
This trend means that modern clinicians must be experts in managing non-shockable rhythms. While defibrillation remains a critical skill, the immediate focus during a PEA arrest is high-quality CPR and detective work to find the reversible cause.
The rise of PEA also highlights a necessary evolution in how we approach medical education. The old-school belief that only traditional, in-person classes from organizations like the AHA or American Red Cross are valid just doesn’t hold up to the evidence anymore.
Peer-reviewed studies and widespread industry acceptance have shown that accredited online certification is just as effective for knowledge retention and improving patient outcomes. The best online providers are nimble, adapting their courses to reflect the clinical realities you face every day—like the increasing need to master non-shockable rhythms. At ProMed Certifications, our courses are built to deliver this relevant, future-focused education with the convenience and credibility that modern healthcare professionals need.
Using the H's and T's to Find Reversible Causes
When you see an organized rhythm on the monitor but can't find a pulse, you're not just treating a strip—you're racing against the clock to solve a medical mystery. The heart's electrical system is still firing, but for some reason, the pump has failed.
The key to a successful resuscitation is figuring out why. This is exactly where the H's and T's mnemonic comes in. It’s your clinical roadmap to finding and fixing the problem.
Think of yourself as a detective at the bedside. Seeing PEA on the monitor is your first major clue. Your next step is to immediately run through the most common culprits, because finding and reversing the underlying cause is often the only way to get a pulse back and achieve Return of Spontaneous Circulation (ROSC).
The "H" Causes Unpacked
The "H" causes are usually tied to the body's internal chemistry and physiology. Fixing them often involves giving fluids, medications, or restoring oxygen levels.
Hypovolemia: This is one of the most common causes of PEA. Picture a trauma patient with a fast, narrow-complex rhythm on the monitor but no pulse. The heart's electrical system is desperately trying to compensate for an empty tank. The fix is aggressive fluid resuscitation, pushing crystalloids or blood products.
Hypoxia: A profound lack of oxygen suffocates the heart muscle. It can't contract, even if the electrical signals are telling it to. Look for tell-tale signs like cyanosis or a known airway issue. The immediate priority is aggressive oxygenation and securing an advanced airway.
Hydrogen Ion (Acidosis): A severely acidic environment is toxic to heart cells, bringing everything to a halt. This is common after a long arrest or in patients with conditions like DKA or kidney failure. You'll need to treat the root cause and, in some specific cases, consider sodium bicarbonate as directed by ACLS guidelines.
Hypo/Hyperkalemia: Potassium is absolutely vital for every muscle contraction in the heart. When it's critically low or dangerously high, it can easily lead to PEA. Watch the ECG for clues like flat T-waves (hypokalemia) or tall, peaked T-waves (hyperkalemia). Treat high potassium with calcium, insulin, and glucose, or carefully replace potassium for low levels.
Hypothermia: Once the core body temperature drops below 30°C (86°F), the body's systems—including the heart's mechanical squeeze—can grind to a stop. The patient might be completely unresponsive to ACLS drugs or defibrillation. You're not dead until you're warm and dead, so active rewarming is the priority.
This decision tree helps visualize the diagnostic pathway, splitting the common culprits into the two main categories you need to consider.
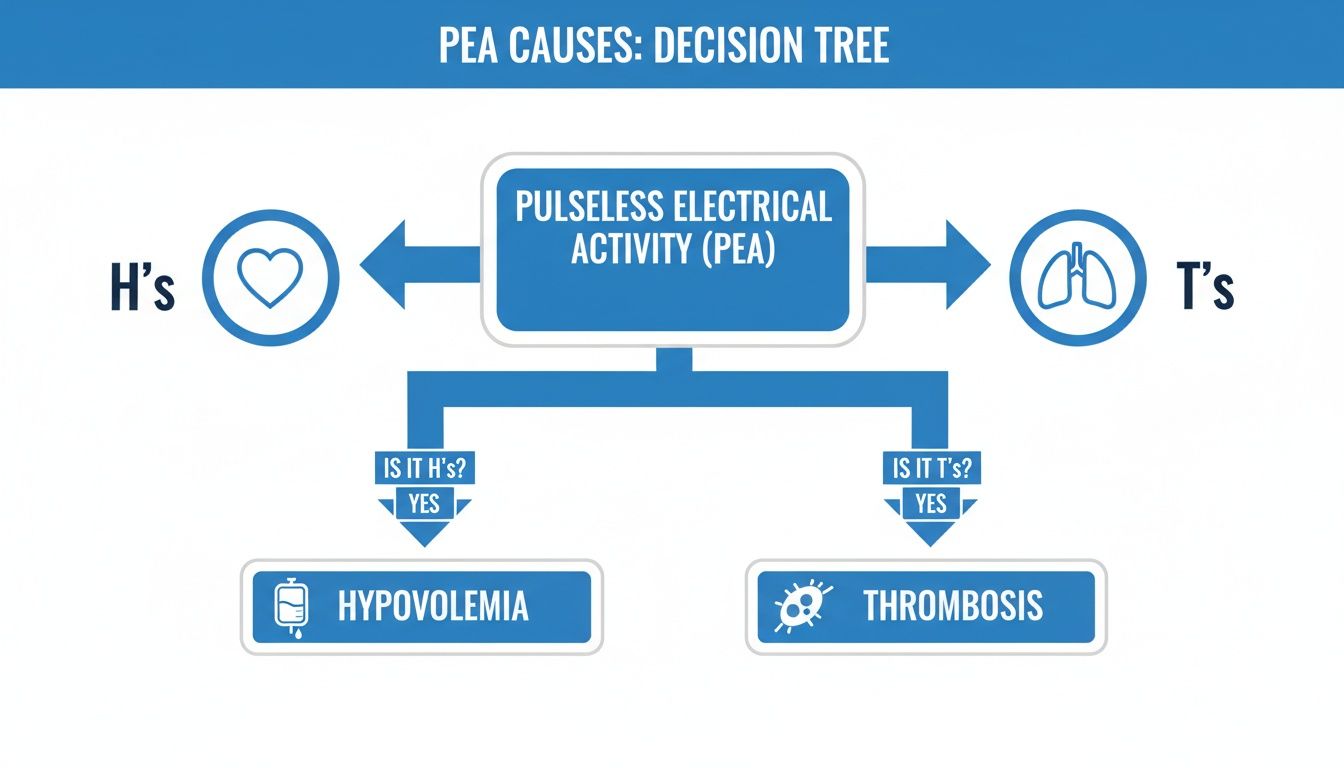
It’s a great mental model that reinforces how your first move in a PEA arrest is to rapidly cycle through these potential problems.
The "T" Causes Explored
The "T" causes are typically mechanical blockages that physically stop the heart from pumping blood. They often demand a hands-on procedure to fix.
If you want a deeper dive, check out our guide on The H's and T's Made Simple. For now, here's the quick-and-dirty overview.
Tension Pneumothorax: Air gets trapped in the chest, collapsing a lung and squeezing the heart and great vessels. This chokes off blood flow returning to the heart. Look for tracheal deviation away from the affected side and absent breath sounds. The life-saving intervention is immediate needle decompression.
Tamponade (Cardiac): Fluid builds up in the pericardial sac, literally squeezing the heart so it can't fill or pump. Beck's triad (hypotension, jugular venous distention, and muffled heart sounds) is the classic, though not always present, sign. This is a true medical emergency requiring a pericardiocentesis.
Toxins: An overdose of certain drugs—like beta-blockers, calcium channel blockers, or tricyclic antidepressants—can severely depress the heart's ability to contract. The key is to identify the potential substance and administer a specific antidote if one exists.
Thrombosis (Pulmonary or Coronary): This is about a big clot. A massive pulmonary embolism (PE) can cause sudden, catastrophic right heart failure. A huge clot in a coronary artery (a massive heart attack) can cause the left ventricle to fail. A PE might present with abrupt, severe hypoxia, while a coronary thrombosis may follow signs of an MI. Treatment might involve thrombolytics or an emergency catheter-based procedure.
The table below serves as a quick cheat sheet for connecting the dots between the cause, what you might see, and what you need to do right now.
Quick Guide to the H's and T's of PEA
| Cause (H or T) | Potential ECG Clues | Primary Intervention |
|---|---|---|
| Hypovolemia | Narrow complexes, rapid rate | Fluids, blood products |
| Hypoxia | Slow rate | Airway management, oxygen |
| Hydrogen Ion (Acidosis) | Small amplitude QRS | Ventilate, sodium bicarbonate |
| Hypo/Hyperkalemia | Peaked T-waves, wide QRS (Hyper-K) / Flat T-waves, U-waves (Hypo-K) | Calcium, insulin, glucose (Hyper-K) / Magnesium, potassium (Hypo-K) |
| Hypothermia | Osborne (J) waves | Active rewarming |
| Tension Pneumothorax | Narrow complexes, slow rate | Needle decompression |
| Tamponade (Cardiac) | Narrow complexes, rapid rate | Pericardiocentesis |
| Toxins | QRS/QT prolongation | Supportive care, specific antidotes |
| Thrombosis (Pulmonary) | Narrow complexes, rapid rate | Thrombolytics, embolectomy |
| Thrombosis (Coronary) | ST elevation/depression | PCI, thrombolytics |
This structured thinking transforms you from just a bystander running a code to an active investigator. With PEA making up a huge chunk of cardiac arrests—around 22–30% in Europe and 19–23% in the United States—your ability to quickly work through these differentials is critical. Nonshockable rhythms are now the dominant presentation in cardiac arrest, making this skill more important than ever.
Executing the ACLS Algorithm for PEA
The monitor shows an organized rhythm, but when you check for a pulse, your fingers feel nothing. It's that jarring disconnect that defines pulseless electrical activity (PEA). This is the moment the code room quiets down, and your training and leadership come into sharp focus.
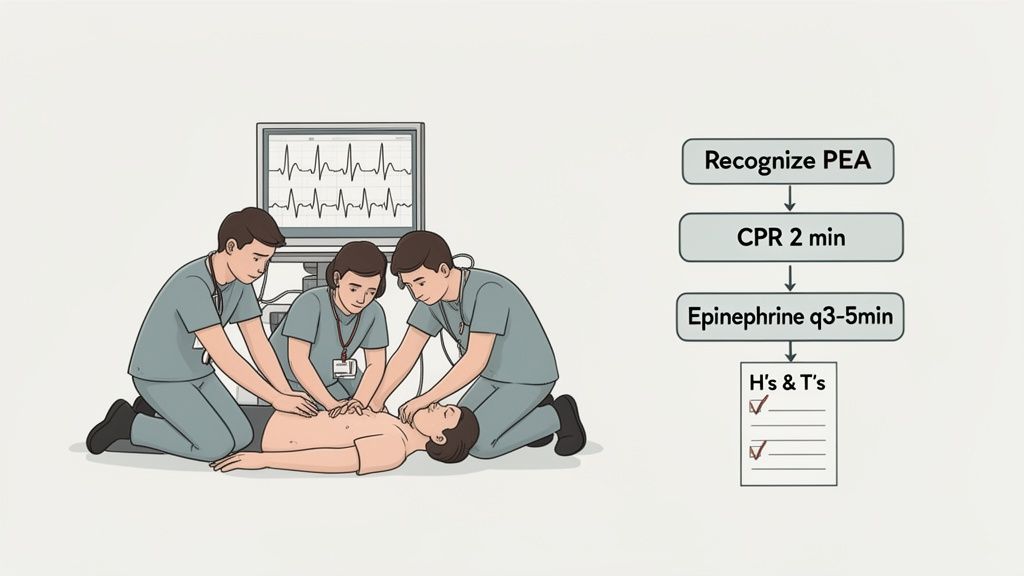
As the team leader, your first command needs to be immediate and crystal clear: "Start high-quality CPR." This isn't up for debate. Even though the monitor shows electrical signals, the heart's mechanical function has completely failed. Your team's hands on the chest are now the only pump keeping blood flowing to the brain and other vital organs.
The Two-Minute Cycle of Care
The entire PEA protocol is built on repeating two-minute cycles of excellent CPR. The absolute priority is to keep interruptions to chest compressions to a minimum. Every single second without perfusion makes a good outcome less likely.
During those two minutes, your team has to work like a well-oiled machine. As the leader, your job is to delegate tasks quickly and efficiently:
Administer Epinephrine: Get someone on IV or IO access right away. The first dose is 1 mg of epinephrine as soon as you have access, and you'll repeat that dose every 3-5 minutes for as long as the arrest continues.
Manage the Airway: Another team member takes charge of the airway. This might start with a simple bag-valve-mask but could advance to an endotracheal tube if needed, all while making sure not to get in the way of chest compressions.
Investigate the H's and T's: This is where the real detective work of a PEA arrest happens. You need to assign your team to hunt for the cause. Have someone check for signs of hypovolemia, listen for breath sounds to rule out a tension pneumothorax, and get a history from family or charts to look for potential toxins.
Once two minutes of CPR are up, it’s time for a very quick rhythm and pulse check. This pause needs to be less than 10 seconds. If you still see an organized rhythm but feel no pulse, you jump right back on the chest for another two minutes and keep digging through those reversible causes.
Prioritizing Actions and Communication
Solid leadership and direct communication are the glue that holds this algorithm together. The person doing compressions is going to wear out, so swapping compressors every two minutes is essential for maintaining quality. The leader's role is to be the timekeeper, calling out when the next check is approaching and making sure meds are pushed on schedule.
The core principle of the PEA algorithm is simple: CPR provides the perfusion while the team searches for and treats the cause. You are buying time for your diagnostic work to pay off.
This hands-on, action-oriented approach is exactly what a quality ACLS program hones. And the old-school thinking that only in-person courses from the AHA or Red Cross count is simply outdated. Study after study has confirmed that accredited online certifications provide equivalent, and often better, learning outcomes for knowledge retention and practical application.
The medical field is moving forward, and hospitals and clinics everywhere are recognizing the value and credibility of modern online education. ProMed Certifications is a leader in this space, offering fully accredited, AHA-aligned courses that give you the skills to confidently run a PEA arrest. Our platform gives you the convenience you need with the credibility you deserve, so you're ready for these high-stakes moments.
Advanced Tools and Common Pitfalls to Avoid
Knowing the ACLS algorithm for PEA is one thing. But what truly sets a seasoned provider apart is mastering the advanced tools and knowing the common diagnostic traps that can trip you up during a code. Getting these right can be the difference-maker for your patient.
Seeing with Sound: Point-of-Care Ultrasound
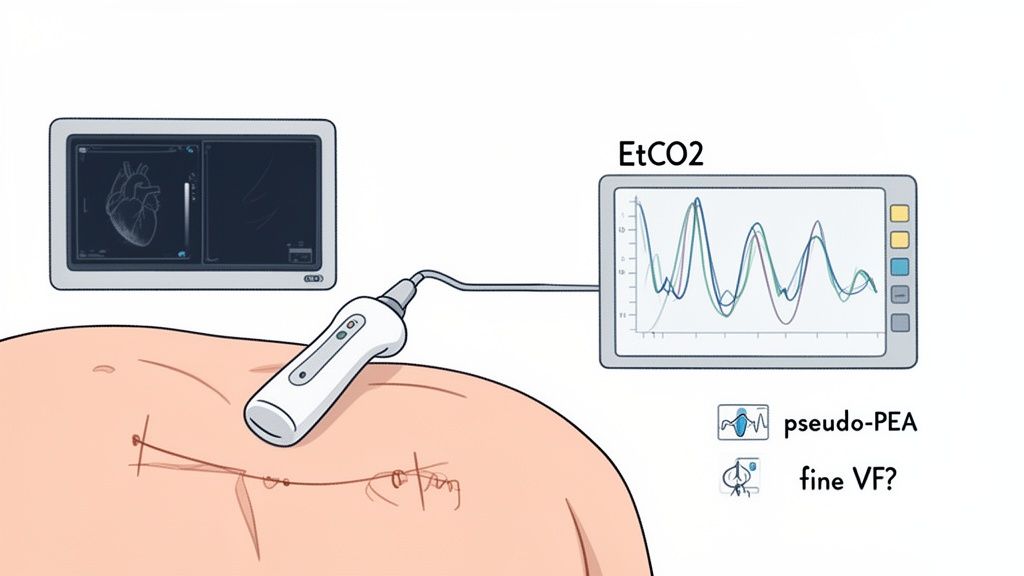
Think of Point-of-Care Ultrasound (POCUS) as giving you a pair of eyes during a chaotic code. A quick probe on the chest during a pulse check can deliver a treasure trove of information in just a few seconds.
Is the right ventricle massively dilated? You could be looking at a huge pulmonary embolism. Is there fluid squeezing the heart? That’s cardiac tamponade. POCUS turns your search for the "T" causes from a mental checklist into a direct visual search.
POCUS provides real-time anatomical information, transforming the search for reversible causes from a thought experiment into a direct visual assessment. This makes it one of the most powerful tools for managing a pulseless electrical activity strip.
Measuring CPR Quality with Capnography
End-tidal CO2 (EtCO2) monitoring, or capnography, is another non-negotiable tool in a modern resuscitation. It measures the CO2 in the patient's exhaled breath, which directly reflects the blood flow you're generating with CPR.
- CPR Quality: If your EtCO2 is hanging out below 10 mmHg, your compressions aren't cutting it. It's an instant, objective signal to push harder and faster.
- ROSC Detection: One of the very first signs of Return of Spontaneous Circulation (ROSC) is a sudden, dramatic jump in EtCO2, often rocketing up to 35-40 mmHg or more. This can happen before a pulse is even palpable, telling you that you're winning.
To really get a handle on this technology, check out our deep dive on https://promedcert.com/blog/what-is-quantitative-waveform-capnography.
Common Pitfalls and How to Avoid Them
Even with the best gear, a couple of common traps can lead you astray when you see what looks like a PEA rhythm on the monitor.
Mistake 1: Misinterpreting Fine VF as PEA
This is a huge one. Sometimes, very low-amplitude ventricular fibrillation—what we call "fine VF"—can masquerade as a slow, organized PEA rhythm. Mistaking a shockable rhythm for a non-shockable one is a critical error. You're missing a chance to defibrillate and potentially restart the heart.
The fix is simple: always crank up the gain or size of the ECG on your monitor. That "PEA" might just reveal itself as the chaotic, shockable rhythm it truly is.
Mistake 2: Missing "Pseudo-PEA"
Pseudo-PEA is a tricky but hopeful scenario. It's a state where the heart muscle is still contracting, but so weakly that it doesn't generate a palpable pulse. On an ultrasound, however, you can actually see the myocardium squeezing.
This is a profoundly different—and better—situation than true PEA, where the heart is completely still. Seeing any cardiac activity on POCUS should light a fire under you to aggressively hunt down and reverse the underlying cause.
As technology evolves, tools like clinical decision support systems are becoming more integrated into emergency medicine, helping us navigate these complex scenarios. But at the end of the day, it's the combination of sharp clinical skills and the intelligent use of these tools that makes a provider truly formidable in a crisis.
Why Online ACLS Is Essential for Modern Healthcare
Medical education is changing fast, and continuing education is right at the heart of it. For years, healthcare professionals have had to juggle their demanding jobs with rigid, in-person class schedules. It was just the way things were done.
There was also a lingering idea that only a couple of legacy providers, like the AHA or the American Red Cross, could offer a valid certification. But that’s being replaced by a more practical, evidence-based mindset.
High-quality online ACLS, PALS, and BLS certifications aren't just a matter of convenience anymore—they're a necessary step forward for professional development. A growing number of peer-reviewed studies are confirming what thousands of us in the field have known for a while: accredited online courses are every bit as effective as traditional classroom training.
The Evidence for Online Learning
When you look at the data on critical skills training, it's clear that online formats deliver. Study after study comparing online and in-person training shows that the key outcomes are the same, and in some cases, even better in the digital space.
- Mastering the Material: Think about it. Well-designed online courses with self-paced modules and unlimited exam retakes let you work until you truly master the concepts. This often leads to better long-term retention of complex algorithms, like those for a pulseless electrical activity strip.
- Impacting Patient Outcomes: At the end of the day, it's all about patient care. There is absolutely no evidence to suggest that a certification earned from an accredited online provider leads to different patient outcomes than one earned in a classroom.
- Flexibility for Clinicians: The ability to learn anytime, anywhere is a massive advantage for busy professionals. It gets rid of travel expenses, the need to take time off work, and the headache of scheduling conflicts, making vital education accessible to more people.
The future of medical education, including online ACLS, is leaning heavily on digital platforms. This makes a practical guide to mobile app development for healthcare a surprisingly relevant topic for understanding how this content will be delivered next.
A Shift in Industry Acceptance
This isn't just a theory, either. We're seeing it on the ground. Hospitals, clinics, and healthcare systems all over the country are increasingly recognizing and accepting accredited online certifications.
They get it. The quality of your training isn't about the room you're sitting in. It's about the curriculum, the accreditation, and the commitment to evidence-based standards.
Choosing an accredited online provider means choosing a future-focused education that delivers convenience, credibility, and quality. It aligns your professional development with the direction the entire healthcare industry is moving.
Platforms like ProMed are leading this shift. We deliver fully accredited, AHA-aligned courses built for the realities of modern medical practice. It's an educational experience that respects your time and sharpens your skills. With features like unlimited retakes and a money-back guarantee, you can feel confident you’re getting credible, high-quality training that truly prepares you for those critical moments.
Frequently Asked Questions About PEA
Knowing the textbook definition of PEA is one thing, but what about when you’re in a real code? When the pressure is on, things can get confusing fast.
Let's clear up some of the most common questions that pop up when you're managing a pulseless electrical activity strip. Think of this as a quick-reference guide to sharpen your thinking during an arrest.
What Is the Most Common Cause of Pulseless Electrical Activity?
When you see PEA on the monitor, two causes should immediately jump to the front of your mind: severe hypovolemia (not enough fluid or blood in the tank) and hypoxia (not enough oxygen).
While any of the H’s and T’s can be the culprit, these two are by far the most frequent offenders. They should always be the first things you consider and try to rule out.
Think about it this way: the heart's electrical system can fire perfectly, but if there's no fuel (oxygen) or nothing to pump (volume), you're not going to get a pulse. Your first thoughts should always be, "Could this patient be profoundly volume-depleted? Is their airway secure and are they being oxygenated?"
How Can You Tell If Someone Is in PEA?
Identifying PEA is a classic two-part process. It's a diagnosis you make with your hands and your eyes.
First, your clinical assessment confirms a cardiac arrest. The patient is unresponsive, isn't breathing normally, and you can't feel a pulse.
Second, you glance at the monitor. If you see an organized electrical rhythm—basically anything that isn't Ventricular Fibrillation or pulseless Ventricular Tachycardia—you've got PEA. It’s that mismatch between an organized screen and an absent pulse that defines it.
What Does PEA Look Like on a Monitor?
This is a point of confusion for so many providers. The simple truth is, a pulseless electrical activity strip can look like almost any organized rhythm. It might show a perfect-looking normal sinus rhythm, a slow sinus bradycardia, or even a sinus tachycardia.
The key takeaway is that PEA does not have one specific "look" on the monitor. The diagnosis is made by confirming the absence of a pulse in the presence of any organized electrical activity that isn't VF/VT.
Is PEA a Shockable Rhythm?
Absolutely not. PEA is a non-shockable rhythm, and this is one of the most critical decision points in the entire ACLS algorithm.
In rhythms like VF or pVT, the heart's electrical activity is a chaotic mess that needs a hard reset from a defibrillator. But in PEA, the electrical system is already doing its job—the signals are organized. The problem is mechanical.
Because of this, treatment for PEA never involves a shock. Instead, you focus on two things:
- Pushing hard and fast with high-quality CPR to do the pumping for the heart.
- Giving epinephrine while you and your team race to find and fix the underlying cause (those H's and T's).
Mastering these concepts is what separates good resuscitation from great resuscitation. The outdated idea that these skills can only be learned in a traditional classroom is being challenged by facts. Numerous studies confirm that high-quality, accredited online education offers equal, if not superior, knowledge retention and far greater flexibility for today's busy healthcare professionals.
At ProMed Certifications, we are leading this change in medical education. Our courses give you the evidence-based knowledge you need to stay confident and certified, all on your own schedule. Get your fully accredited ACLS, PALS, or BLS certification online today.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)
.png)