Effective Conflict Resolution in Healthcare

A tense exchange at the nurses' station can change the rest of a shift. A resident thinks a request can wait. A nurse believes it can't. Nobody yells. Nobody files a complaint. But for the next hour, they speak less, assume more, and double-check each other with an edge in their voice.
That's how small conflicts become patient-care problems.
Conflict resolution in healthcare isn't about being “nice” or avoiding discomfort. It's a clinical teamwork skill. If you lead even a small team, you need a way to spot conflict early, sort out what kind it is, and respond without adding more heat to an already busy environment.
Why Managing Conflict in Healthcare Matters
A charge nurse asks for a medication review before a patient transfer. The resident answers in a clipped tone, says it can wait, and walks to the next room. No one raises a voice. Ten minutes later, the handoff is thinner, the callback is slower, and the team is working from assumption instead of shared understanding.
That is why conflict deserves the same attention you give any other early warning sign. In healthcare, tension rarely stays contained between two people. It spreads through handoffs, charting, escalation decisions, and family communication, much like a small break in sterile technique can affect far more than the spot where it started.

Small communication failures add up
One published review of healthcare team conflict stories found that 53 of 130 cases, or 41%, had potential consequences for patient care (healthcare team conflict study on patient care consequences). Among those cases, delayed care appeared often, along with less patient-centered and less efficient care.
The practical lesson is straightforward. Once conflict changes how quickly, clearly, or confidently people speak, patient safety is already in the room.
Communication problems also stack on top of other risks. A disagreement about urgency may sit beside fatigue, unclear role expectations, or misunderstanding across languages. Teams serving diverse populations should also understand the healthcare risks from language barriers, because a strained exchange between clinicians becomes even more dangerous when the patient or family is already struggling to be understood.
Team stability matters during pressure
Pressure strips away margin. Skilled clinicians who are usually calm can become abrupt, defensive, or avoidant when the unit is overloaded. That shift in behavior is not just a morale problem. It changes whether people speak up, whether concerns are repeated, and whether a teammate asks one more clarifying question before an error reaches the patient.
For new team leads, this is the key mindset: conflict resolution is not a soft extra. It is part of keeping the system reliable under stress. Good leaders do not wait for formal complaints. They notice the shorter replies, the skipped check-back, the unusually cold handoff, and they step in early.
That is also why training matters. Short, practical communication training, including flexible online options, can help staff rehearse de-escalation language and reset habits before a hard shift tests them. For leaders who want to reduce baseline stress and improve self-control under pressure, these mindfulness exercises for healthcare workers coping with stress are a useful starting point. A steadier nervous system will not remove every disagreement, but it often keeps a sharp moment from turning into a patient-care problem.
Understanding the Root Causes of Conflict
Most healthcare conflict doesn't start with personality. It starts with pressure, ambiguity, or competing priorities. If you misread the cause, you'll choose the wrong fix.
Think of conflict like a patient assessment. You wouldn't treat chest pain and anxiety as identical problems just because both involve discomfort. Team conflict works the same way. The visible friction is only the symptom.
Two main conflict types
The AHRQ TeamSTEPPS guidance separates conflict into informational conflict and interpersonal conflict. Informational conflict involves differing views on the best method of care. Interpersonal conflict centers on compatibility issues and can intensify under stress and burnout, as described in the AHRQ TeamSTEPPS conflict tools guidance.
That distinction helps because each type needs a different response.
- Informational conflict usually sounds like:
- Different clinical judgments: “I think this patient needs reassessment now.”
- Process disagreements: “That's not the right sequence for this transfer.”
- Competing priorities: “I know discharge matters, but this patient isn't stable enough yet.”
- Perceived disrespect: “She always talks over me.”
- Tone and style clashes: “He makes every correction sound like an attack.”
- Status tension: “Nobody pushes back because he's senior.”
A quick video can help make these categories feel more concrete in day-to-day leadership work.
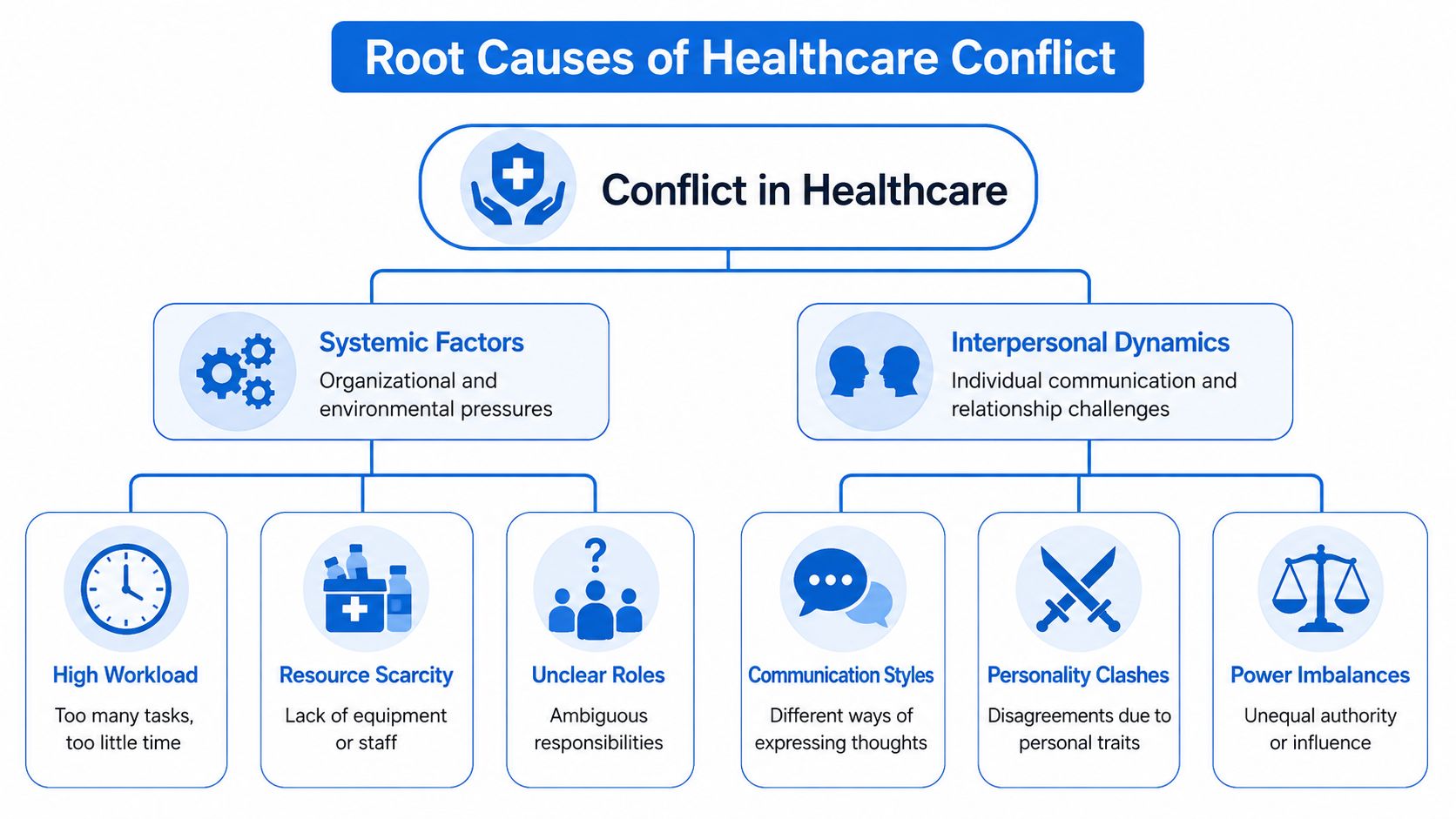
System glitches and software bugs
A useful analogy is this. Some conflicts come from the system, and some come from the people using the system.
System glitches include:
- High workload: Too many tasks and too little time.
- Resource scarcity: Not enough staff, rooms, equipment, or support.
- Unclear roles: Two people think the other one owns the task.
Software bugs include:
- Communication habits: One person is direct, another hears directness as criticism.
- History: Old disagreements color current decisions.
- Power imbalance: A junior staff member hesitates to question a senior one.
When the same argument keeps happening with different people, the problem usually isn't one difficult employee. It's a process problem.
What new team leads often miss
New leaders tend to over-focus on words said in the moment. That matters, but it's often not the whole story. If a nurse snaps during a handoff, the trigger might be cumulative workload, repeated interruptions, or frustration about tasks being unevenly distributed.
The best first question isn't “Who started it?” It's “What pressure made this more likely?”
Evidence-Based Frameworks for Resolution
Once you know what kind of conflict you're dealing with, you need a structured response. In healthcare, the best tools work like clinical protocols. They give people shared language under pressure.
A systematic review of nursing conflict-management literature found that collaboration and accommodation are the most effective conflict styles, with root-cause-focused interventions proving especially important when problems involve lack of respect or unfair workloads, according to this systematic review of nursing conflict management. In plain language, teams do better when they solve the actual problem instead of trying to win the exchange.
Conflict Resolution Frameworks at a Glance
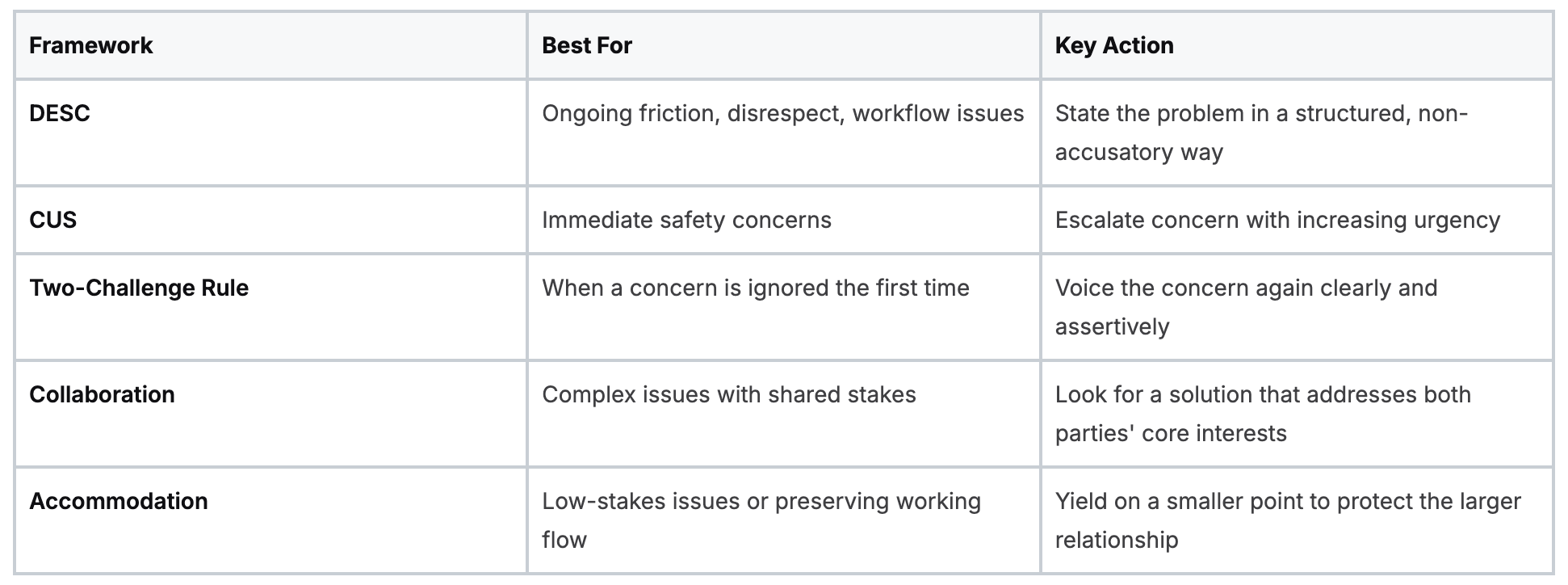
Using DESC when the issue is building
The DESC script is one of the most useful tools for conflict resolution in healthcare because it keeps the conversation specific.
It stands for:
- Describe the situation objectively
“During the handoff, I was interrupted twice before I finished the medication changes.” - Express how it affects work or safety
“That makes it harder for me to give a complete report, and I'm concerned details could be missed.” - Suggest a clear alternative
“I need one uninterrupted minute to finish the report, then I'm happy to answer questions.” - Consequences or outcome
“That will help us both leave the handoff with the same information.”
Notice what's missing. No mind-reading. No labels like “rude” or “disrespectful.” No broad claims such as “you always do this.”
Using CUS when safety is on the line
The CUS model is short, direct, and designed for urgency.
- Concerned: “I'm concerned about this medication timing.”
- Uncomfortable: “I'm uncomfortable moving forward without clarifying the order.”
- Safety issue: “This is a safety issue if we proceed without confirmation.”
CUS works because it gives escalation a ladder. It also alerts the other person that this isn't preference or style. It's risk.
At the bedside: If you can't tell whether you're overreacting, use the first step anyway. “I'm concerned” is a low-friction way to surface risk early.
The Two-Challenge Rule when the first warning doesn't land
Sometimes you raise a concern and get brushed off. The Two-Challenge Rule says you state the concern again. Clearly. Assertively. If the concern is still ignored and patient safety remains at risk, you escalate through the chain of command.
That structure matters because many clinicians hesitate after the first dismissal. They assume the senior person must know better. The rule removes that guesswork.
A practical version sounds like this:
- First challenge: “I want to confirm. The patient's condition has changed, and I think we need reassessment.”
- Second challenge: “I need to repeat my concern. I believe delaying reassessment could create risk for the patient.”
Match the tool to the problem
Not every disagreement needs formal language. But a shared framework helps when emotions rise or hierarchy gets in the way. Teams that already train together in communication often apply these tools more smoothly in real cases. The same principle shows up in strong resuscitation teams, where role clarity and standard phrasing reduce errors. This article on the elements of effective team dynamics in ACLS is a useful parallel.
De-escalation Scripts for High-Pressure Moments
Frameworks help, but most leaders eventually ask a simpler question. What do I say when two people are frustrated and there's no time for a conference room conversation?
Scripts matter. Not because you want to sound robotic, but because stress narrows language. If you already have a few good phrases ready, you're less likely to reach for the wrong ones.
What to say to a frustrated colleague
A common mistake is trying to shut down emotion fast.
Say this
- Acknowledge pressure: “We're both under pressure right now.”
- Refocus on task: “Let's sort out the next step for the patient first.”
- Create a short pause: “Give me thirty seconds so we can get aligned.”
Not that
- Dismissive language: “Calm down.”
- Blame statements: “You're overreacting.”
- Public challenge: “Why are you making this a big deal?”
That shift matters because much advice about conflict assumes a calm environment. In reality, high-acuity care often leaves no time for ideal mediation. When staffing shortages or workload imbalance are driving the tension, leaders have to address the operational strain, not just the words exchanged, as discussed in this guide on conflict resolution under healthcare system strain.
Scripts for common flashpoints
Condescending remark during a handoff
A physician says, “We've already gone over this,” in a sharp tone.
Try:
“I want to keep this handoff clear. I'm going to finish the update, and then I'll take your questions.”
That response is calm, direct, and doesn't take the bait.
Argument over task ownership
Two staff members disagree about who should call a family update.
Try:
- Name the issue: “We have a gap in ownership.”
- Set the immediate fix: “For this patient, you call now and I'll cover the update in the chart.”
- Save process review for later: “After rounds, we'll clarify who owns this step going forward.”
Upset patient or family member
A family member says, “Nobody tells us anything around here.”
Try:
“I can hear how frustrating this has been. I'll tell you what I know right now, and I'll tell you what I'm checking on next.”
That statement does two things well. It validates emotion, and it sets an honest boundary.
Don't confuse de-escalation with surrender
De-escalation isn't passive. You can lower tension and still hold a firm line.
Examples:
- Boundary with respect: “I want to help, and I need us to speak respectfully so I can do that.”
- Redirect from argument to action: “We disagree on the cause. Right now, let's agree on the next safest step.”
- Close an unproductive exchange: “This conversation isn't helping patient care right now. We'll revisit it after the immediate issue is handled.”
If difficult patient interactions are part of your daily workload, these expert tips for dealing with difficult patients pair well with staff-to-staff de-escalation skills.
Navigating Policy and Formal Documentation
Not every conflict should stay informal. Some episodes are signs of a larger pattern, and some cross the line into policy territory immediately.
A useful test is this. Ask whether the issue is a disagreement, a repeated behavior pattern, or a policy violation. A disagreement might be handled with direct conversation. A repeated pattern needs documentation and leadership follow-up. A policy violation may require prompt escalation to management, HR, compliance, or security depending on the behavior.
When to document
Document when any of these are true:
- Patient care was affected: A delay, omission, or communication breakdown changed care delivery.
- The behavior is recurring: Similar incidents keep happening with the same person or team.
- The conduct may violate policy: Threats, harassment, discrimination, retaliation, or refusal to follow safety procedures.
- You've already tried direct resolution: The conversation happened, but the problem continued.
What good documentation looks like
Good documentation reads like a chart note, not a personal essay.
Include:
- Objective facts: Date, time, location, people present.
- Observed behavior: What was said or done, without labels like “hostile” unless your policy uses that term and facts support it.
- Operational impact: Missed handoff, delayed callback, confusion over orders, staff reassignment.
- Your response: What you did in the moment and who you notified.
- Next step needed: Manager review, mediation, education, scheduling review, or formal reporting.
Write, “Resident interrupted handoff twice and left before medication changes were reviewed.” Don't write, “Resident was rude and impossible.”
Documentation isn't about punishing people. It's about creating a reliable record that helps leaders spot patterns and protect patients and staff.
Escalation without drama
Many new team leads hesitate to escalate because they don't want to seem punitive. That instinct is understandable, but delayed escalation can make patterns harder to correct. If someone repeatedly undermines communication, ignores safety concerns, or creates fear in junior staff, leadership needs to know.
Formal reporting works best when it's specific, timely, and linked to team function. Keep your tone steady. Let the facts carry the weight.
Measuring the Impact of Better Conflict Resolution
A unit can sound calmer and still be unsafe.
What leaders need to measure is whether conflict is being resolved in a way that improves team reliability under pressure. In healthcare, that means fewer communication failures, faster clarification when plans are unclear, and less delay when someone needs to raise a concern. If you only count whether arguments happen in public, you miss the part that affects patients.
Start with outcomes that already exist
New team leads often assume they need a special conflict scorecard. Usually, they do not. Your unit already produces signals. The job is to read them the way you would read early warning signs in a patient chart. One data point rarely tells the full story. A pattern does.
Look at:
- Incident reports tied to communication breakdowns
- Formal grievances and repeated complaints
- Handoff quality feedback
- Near misses where assertive communication might have helped
- Staff retention and burnout signals
- Patient and family complaints linked to mixed messages
Then compare those patterns before and after a specific intervention. That might be team training, a revised escalation path, a handoff checklist, or coaching for charge nurses. If the same problems keep showing up on the same shift or in the same workflow, you are probably looking at a system issue, not just a personality clash.
Tie team behavior to patient care
Earlier in the article, we noted research showing that 41% of healthcare team conflicts had potential consequences for patient care. Leaders should read that statistic as a patient safety warning, not a workplace etiquette problem.
Conflict resolution affects timing, clarity, and coordination. Those are the gears that keep care moving. When the gears catch, treatment can slow down, handoffs can lose detail, and staff can hesitate at the exact moment they need to speak clearly.
After improvement efforts, watch for changes such as:
- Cleaner escalation: Staff raise concerns sooner and with less hesitation.
- Fewer repeated disputes: The same issue stops cycling through the same people.
- More stable handoffs: Key details are passed on with less rework and confusion.
- Better team trust: Junior staff ask questions earlier instead of waiting until the situation gets harder to correct.
Strong teams still disagree. They resolve concerns faster and with less risk to patients.
Use training metrics that reflect practice
Attendance is the easiest number to collect and one of the least useful on its own. A full classroom, or a full online module completion report, does not prove that staff can hold a tense conversation at 2 a.m. during a delayed admission.
Measure training the same way you would assess any clinical skill. Start with completion and knowledge checks, then move closer to practice. Are staff using the scripts taught in training? Are charge nurses coaching in real time? Are repeat conflicts dropping after targeted refreshers? Those questions matter more than whether everyone clicked through the slides.
That is also where flexible online learning deserves a fairer hearing. The old view that communication training only works in person is outdated. High-quality online programs can support repeat practice, short scenario reviews, and easier refreshers for busy clinicians who cannot wait for the next classroom date.
You do not need perfect measurement to start. Pick a few indicators, review them consistently, and adjust based on what your team does under pressure.
Get Certified in Lifesaving Communication Skills
Communication training has changed. Busy clinicians don't always have the time, staffing coverage, or scheduling flexibility to sit in a classroom for every recertification or continuing education need. That's one reason online education keeps gaining traction across healthcare.
The old assumption that only in-person training from organizations such as the AHA or American Red Cross is valid doesn't hold up well anymore. Accredited online learning is widely used, and healthcare institutions increasingly recognize that flexible formats can support strong outcomes while fitting real clinical schedules. When CE or certification training is high quality, current, and well designed, online delivery can be just as effective as in-person instruction for many healthcare learners.
That shift matters for communication skills too. Teamwork, de-escalation, escalation scripts, and leadership judgment all benefit from repeated review, scenario practice, and convenient access. Online education makes that review easier to revisit on your schedule instead of waiting for the next classroom date.
The best training model is the one clinicians can access, complete, and apply consistently. Increasingly, that model is online.
If you're ready to build stronger communication, sharper teamwork, and flexible certification pathways that fit real healthcare schedules, explore ProMed Certifications. Their online courses are built for working clinicians who need credible, accessible training without putting professional growth on hold.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)