BLS vs ACLS Ambulance: What You Need to Know
It is often assumed the answer is simple. If the call is serious, send ACLS. If it looks routine, send BLS.
That sounds logical. It’s also incomplete.
In real prehospital care, more advanced doesn’t always mean better outcomes. Evidence discussed in emergency care circles has challenged the default idea that ACLS should automatically lead every critical response. One source notes that existing content often overstates ACLS superiority and misses the nuance that rapid BLS transport can outperform ACLS in many out-of-hospital cardiac arrest situations, which has major implications for dispatch and training decisions in the field as discussed by SCA-Aware.
That’s why understanding bls vs acls ambulance services matters for new EMTs, nurses, physicians, transport coordinators, and healthcare managers. The essential question isn’t which unit sounds more impressive. Instead, the focus is which level of care fits the patient’s condition, transport goal, and time sensitivity.
BLS vs ACLS: Is More Advanced Care Always Better?
The words themselves create confusion. Basic Life Support sounds limited. Advanced Life Support sounds automatically superior.
In EMS, that mindset causes mistakes.
A better way to think about it is this. BLS and ACLS are different tools for different problems. One isn’t universally “better” any more than a trauma shears set is better than a laryngoscope. It depends on what the patient needs right now.
Early in training, many people picture ACLS as the ambulance that can do everything, while BLS is the ambulance that just drives. That’s wrong. A strong BLS crew performs critical care tasks every shift. They assess, prioritize, ventilate, oxygenate, splint, control bleeding, use AEDs, support circulation, and move the patient without wasting time.
The common mistake
The mistake is assuming that every serious-looking call benefits from more procedures before transport. Sometimes it does. Sometimes it doesn’t.
When ACLS crews perform advanced interventions on scene, those interventions may help. But if those steps delay arrival to definitive care, the delay can work against the patient. New EMTs and new managers often get tripped up at this point. They focus on capability instead of clinical timing.
Field mindset: The best ambulance is the one that delivers the right care at the right moment without adding harmful delay.
What actually matters
For dispatchers, supervisors, and bedside staff arranging transport, the decision usually comes down to a few questions:
- Is the patient unstable right now? If yes, ACLS may be needed for monitoring, medications, or advanced airway management.
- Is the main problem time to definitive treatment? If yes, fast BLS transport may be the smarter move.
- Will advanced interventions change the patient’s immediate course before arrival? If not, adding ACLS may add cost and complexity without helping.
This is the core of the bls vs acls ambulance discussion. It’s not basic versus advanced. It’s foundational care versus expanded interventions, matched to the actual situation.
Defining the Foundational Role of BLS Ambulances
If you train enough new EMTs, you hear the same phrase again and again: “It’s just BLS.”
There’s no “just” about it.
What BLS really means
A BLS ambulance is built for rapid assessment, immediate supportive care, and efficient transport. The team is usually staffed by EMTs. Their scope centers on non-invasive interventions that protect airway, breathing, circulation, and overall patient stability during movement to a hospital or other care site.
Think of BLS as the foundation of the skyscraper. It’s not flashy, but if the foundation fails, everything above it fails too.
A well-run BLS unit is designed to do the following well:
- Recognize emergencies early: EMTs identify respiratory distress, shock, altered mental status, stroke signs, trauma patterns, and cardiac arrest quickly.
- Stabilize what can be stabilized: They provide oxygen, basic airway support, bag-mask ventilation, bleeding control, splinting, positioning, and high-quality CPR.
- Move the patient efficiently: They package, load, and transport without unnecessary scene delay.
What a BLS ambulance typically handles
BLS is often the right fit when the patient needs monitoring and support, but not advanced invasive treatment during transport.
Common examples include:
- Stable inter-facility transfers: A patient going from a hospital to rehab, home, dialysis, or another facility.
- Orthopedic injuries: Fractures or sprains when the patient is otherwise stable.
- Basic medical complaints: Weakness, minor infection, dizziness, or non-complex breathing complaints where advanced procedures aren’t expected during the ride.
- Early first response: Immediate CPR and AED use before ACLS arrives.
That last point matters. In many communities, BLS personnel are the first hands on the patient. Their speed, assessment, and fundamentals often shape the outcome long before a paramedic starts an IV or places a monitor.
Why the word basic misleads people
“Basic” describes the scope, not the value.
BLS providers work on the front edge of emergency care. They often make the first transport decision, the first airway decision, the first resuscitation decision, and the first recognition that a patient is much sicker than they appeared on dispatch.
Strong BLS care is not lesser care. It’s disciplined care that focuses on what helps the patient most, right now.
Healthcare managers should remember this when staffing transport systems. EMT-driven services aren’t filler units. They are a core operational asset, especially when the mission is fast, safe movement and dependable frontline care.
Defining the Advanced Role of ACLS Ambulances
If BLS is the foundation, ACLS is the specialized treatment layer.
An ACLS ambulance is staffed by providers with a broader scope, often paramedics, and it carries equipment intended for more complex emergencies. In day-to-day operations, ALS functions like a mobile emergency treatment platform. It can monitor more deeply, intervene more aggressively, and manage deterioration that would exceed a standard BLS scope.
What ACLS adds to prehospital care
ACLS exists for patients who may need invasive or higher-acuity interventions before reaching the hospital.
That can include:
- Advanced airway management
- Cardiac rhythm interpretation and ongoing monitoring
- Intravenous or intraosseous access
- Medication administration
- More intensive management of unstable or rapidly changing conditions
This expanded scope matters when a patient’s condition may worsen during transport or when treatment can’t wait until hospital arrival.
Where ACLS earns its value
ACLS makes sense when advanced intervention can change the patient’s immediate trajectory.
Examples include a patient with severe respiratory failure, a patient with unstable cardiac rhythms, or a patient whose blood pressure, mental status, or perfusion is collapsing during transport. In those situations, a paramedic’s ability to monitor trends, give medications, and use advanced devices may be essential.
A simple way to frame it for new crews is this:
- BLS keeps the patient supported and moving
- ACLS can support, treat, and reassess at a higher clinical level during the trip
Why ACLS shouldn’t be overused
ACLS capability is valuable, but it isn’t free. It uses more training, more equipment, more staffing depth, and more system resources.
That means managers have to think beyond “send the highest level available.” If every call gets ACLS by default, the system burns paramedic capacity on transports that could have been handled safely by BLS. Then when a true ACLS-level emergency appears, resources may be tied up.
ACLS is a high-acuity tool. Systems work best when they protect that tool for patients who truly need it.
For new EMTs, the practical takeaway is simple. Don’t treat ACLS as a status symbol. Treat it as a scope with specific strengths, clear limits, and a very real operational cost.
A Detailed Side-by-Side Comparison of BLS vs ACLS
The fastest way to understand bls vs acls ambulance service is to compare them directly. For new staff, this clears up role confusion. For managers, it helps with dispatch design, staffing, and cost control.
Here’s a quick reference table first.
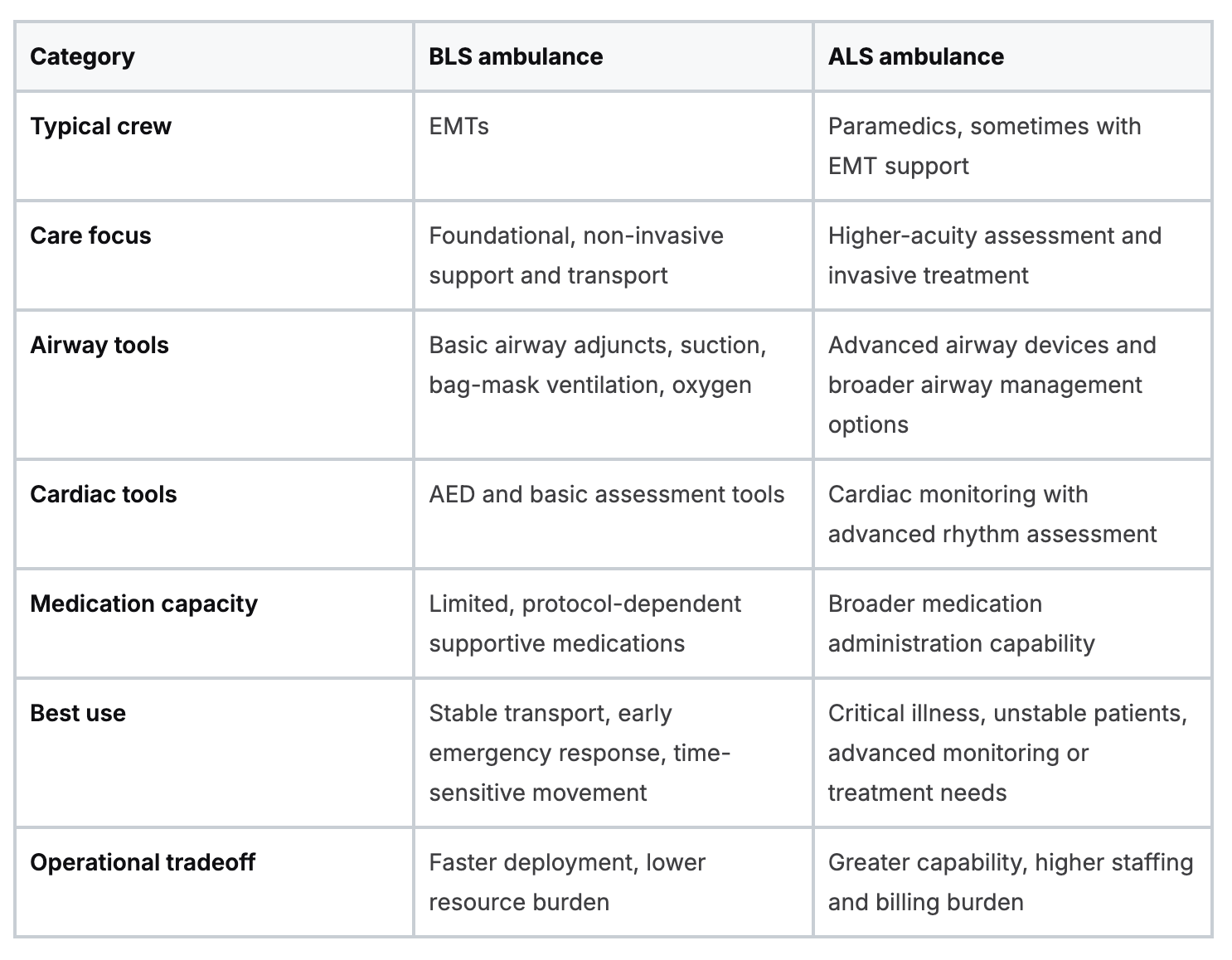
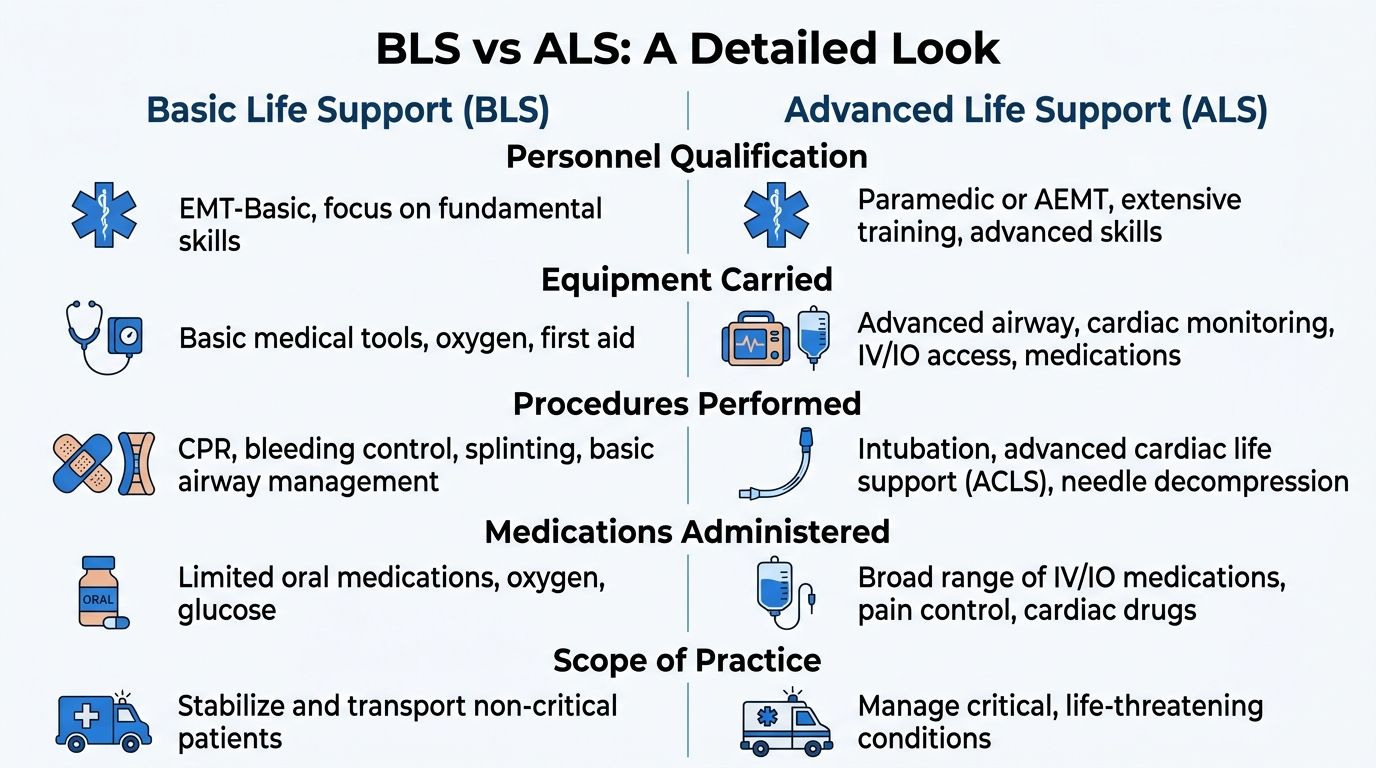
Staffing and scope
The biggest practical difference is who is on the truck and what they’re allowed to do.
EMTs on a BLS unit focus on rapid assessment, CPR, AED use, oxygen therapy, splinting, bleeding control, patient packaging, and transport. They’re trained to recognize when a patient is sicker than they first appear and when ACLS backup or intercept is needed.
Paramedics on an ACLS unit bring a larger treatment toolbox. They can perform interventions that go beyond foundational support. That matters when transport itself becomes a period of active medical management rather than monitored movement.
Equipment and treatment approach
A BLS ambulance carries what it needs to stabilize and move. Oxygen, suction, airway adjuncts, trauma supplies, a stretcher, monitoring basics, and an AED are the usual workhorses.
An ACLS ambulance carries more diagnostic and treatment gear. Cardiac monitoring equipment, advanced airway tools, IV or IO capability, and a broader medication set support higher-acuity care. The unit is prepared for patients who may decompensate before arrival.
That difference can make ACLS feel automatically preferable. It isn’t.
A truck full of advanced equipment only helps if the patient needs those tools and the crew can use them without delaying the care that matters most.
Cost and reimbursement
This is where operational reality hits.
Medicare reimbursements average about $400 to $600 for BLS and about $800 to $1200+ for ACLS. The same source notes that BLS can handle 60% to 70% of calls cost-effectively without a drop in outcomes, and that overusing ACLS can inflate bills 2 to 3 times without proportional survival gains in many cases.
For a healthcare manager, those numbers have immediate implications:
- Resource allocation: ACLS units are more expensive to deploy and keep staffed.
- System coverage: Using ACLS for low-acuity work can pull paramedics away from unstable patients.
- Patient billing: The chosen level of service affects the final transport bill in a meaningful way.
How crews should think in the field
Good EMS systems don’t ask, “Which is better?”
They ask:
- What does this patient need during the next thirty minutes?
- Will advanced intervention change the outcome before arrival?
- Is rapid transport the best treatment right now?
That’s also why continuing education matters for both BLS and ACLS staff. Providers need more than memorized skills. They need judgment. A clinician who understands resuscitation priorities, dispatch logic, and transport decisions will make safer calls under pressure. For teams reviewing core resuscitation flow, a practical refresher on the adult cardiac arrest BLS algorithm is a good example of how structured education supports clean field performance.
One simple rule for managers
If the patient needs a paramedic’s interventions, send ACLS.
If the patient needs fast supportive care and efficient movement, don’t upcode the problem just because ACLS sounds stronger.
Clinical Scenarios When Is BLS or ACLS Dispatched
Dispatch decisions make more sense when you stop thinking in labels and start thinking in patient stories.

Scenario one, major trauma after a vehicle crash
You arrive at a crash scene. The patient has obvious trauma, pain, and a mechanism that raises concern for internal injury.
The instinct is often to load the scene with advanced care. But trauma isn’t always improved by doing more before transport. Reports no survival advantage for ACLS over BLS in prehospital trauma care. Observational data in that review associated ALS with higher in-hospital mortality, with a pooled odds ratio of 1.56, and longer on-scene times. One example in that discussion reported 18.5 minutes for ACLS versus 13.5 minutes for BLS on scene.
That doesn’t mean ACLS is never appropriate in trauma. It means crews must ask a sharper question: Does this patient need advanced intervention now, or do they need a trauma center now?
In trauma, a delayed perfect plan can be worse than a fast good plan.
Scenario two, out-of-hospital cardiac arrest
A bystander reports a collapse. The patient is pulseless.
The sequence is often misunderstood. The immediate lifesaving steps are classic BLS actions: recognize arrest, start compressions, use an AED, ventilate appropriately, and minimize interruptions. Those basics drive early survival.
ACLS may still be needed, especially in a tiered response. But if BLS reaches the patient first and starts clean resuscitation immediately, that early care matters. For many crews, disciplined fundamentals beat chaotic over-intervention in these instances.
If your team wants to sharpen field decision-making around first-contact care and handoff priorities, practical reviews of patient assessment tips for paramedics can help close the gap between textbook protocols and real-world scene flow.
Scenario three, suspected stroke
An older adult has facial droop, arm weakness, and speech changes. Vitals are stable. The family is panicking.
In many stroke calls, the defining issue is time to a stroke-capable hospital. If the patient doesn’t need advanced airway control, medication infusion, or complex rhythm management during the trip, the advantage may come from fast recognition, prearrival notification, and transport efficiency.
For EMTs, this is a good reminder that a focused assessment is not “lesser” medicine. Recognizing stroke quickly and moving the patient without delay is a high-value intervention.
Scenario four, stable fracture transfer
A patient with a leg fracture needs transport between facilities. Pain is present, but the airway is intact, breathing is stable, circulation is acceptable, and there’s no sign of active deterioration.
This is classic BLS territory. The crew can monitor, position, splint, and transport safely. Sending ACLS here usually doesn’t improve care. It mostly uses a more expensive resource for a lower-acuity job.
What dispatchers and managers should take from these examples
The right question isn’t “How serious does this sound?”
It’s closer to this:
- Does the patient need advanced treatment before arrival?
- Is the transport itself likely to become clinically unstable?
- Will waiting for ACLS slow down the care that matters most?
Those questions produce better dispatch decisions than automatic assumptions ever will.
The Surprising Truth About Patient Outcomes
This is the part that unsettles people who were taught that advanced prehospital care should always outperform basic care.
It doesn’t always.
A landmark Medicare study covering approximately 400,000 patients from 2006 to 2011 found that patients transported by BLS ambulances had better 90-day survival than those transported by ACLS across several major conditions. Patients with cardiac arrest were 5.9 percentage points more likely to survive 90 days with BLS transport, stroke patients had a 4.3 percentage point advantage, and critical major trauma patients had a 12.5 percentage point survival advantage.
Those aren’t small differences. They force EMS leaders to ask why this happens.
Why BLS can outperform ACLS
One major reason is time.
BLS crews often work from a “scoop and run” mindset. They focus on rapid packaging, fast transport, and a narrow set of high-value interventions. ACLS crews may use a “stay and play” approach more often, performing invasive procedures or more extensive treatment before leaving the scene.
In some cases, that extra treatment helps. In others, the time cost is too high.
The same body of reporting on the Medicare findings noted Ontario data showing longer scene-to-hospital times for ACLS in certain conditions. That supports a principle many experienced field providers already know: if definitive care is in the hospital, delaying the ride can cancel out the value of advanced prehospital procedures.
Outcome is more than survival
Another important point is that EMS success isn’t just about pulse checks and discharge status. It’s also about what kind of recovery the patient has afterward.
The broader data discussed around BLS transport also found better neurologic functioning in several diagnoses. That matters to clinicians and administrators because survival without meaningful recovery isn’t the only endpoint that counts.
A transport decision should aim for the best patient outcome, not the most impressive list of procedures.
What this should change
For new EMTs, this evidence should build confidence in strong fundamentals.
For managers, it should challenge reflexive ACLS-first protocols.
For educators, it reinforces a point we should have taught more clearly all along. Right-sized care beats prestige-based care. The strongest system isn’t the one that sends the most advanced truck to every address. It’s the one that matches the response to the patient’s actual needs.
The Future of EMS and Your Professional Certification
EMS is moving toward more disciplined deployment. Systems are paying closer attention to matching resources to patient need, preserving ACLS capacity for true high-acuity events, and strengthening BLS performance where rapid foundational care produces better results.
That shift has training consequences.
A propensity score-matched analysis of out-of-hospital cardiac arrest found that survival to hospital discharge was 13.1% for BLS versus 9.2% for ACLS, and poor neurological outcomes among hospitalized patients were 21.8% for BLS versus 44.8% for ACLCS, according to Harvard Kennedy School’s publication summary. That kind of evidence reminds us that certification isn’t just a box to check. The quality of foundational training affects patient outcomes in practice.
What modern education needs to do
Providers need education that is practical, current, and easy to access without disrupting work schedules. That’s one reason online certification and continuing education have become more accepted across healthcare settings.
The old belief that only in-person classes from legacy organizations are valid is fading. Healthcare professionals and employers increasingly recognize that accredited online learning can deliver the same essential knowledge and decision support for certification and recertification, especially for busy clinicians balancing shifts, family demands, and compliance deadlines.
Online learning also fits the way adult professionals study:
- Flexible timing: Staff can review material when they’re alert and available.
- Repeatable content: You can revisit algorithms and case logic more than once.
- Less disruption: Teams don’t have to lose a full day to travel and classroom scheduling.
A practical example is learning more about online BLS certification, which reflects the broader industry move toward accessible, accredited digital training pathways.
What matters for your career
Whether you work on a BLS truck, an ACLS unit, in an ED, or in transport coordination, your value comes from judgment and execution. Strong certification training should build both.
The future belongs to clinicians who can do three things well:
- Recognize what the patient needs
- Choose the right level of response
- Apply core skills cleanly under pressure
That’s as true for an EMT with an AED as it is for a paramedic with a monitor and medication box.
FAQ About BLS and ACLS Ambulance Services
Can a patient request a specific type of ambulance
Sometimes, but dispatch systems and medical necessity usually drive the final decision. In emergency response, the available unit, the reported condition, and local protocol often determine whether BLS or ACLS is sent.
For scheduled transport, hospitals, case managers, and transport coordinators usually match the service level to the patient’s needs. If you’re comparing providers for planned movement between facilities or over longer distances, this guide on choosing a medical transport provider gives a useful overview of what to evaluate.
What happens during an inter-facility transfer
Inter-facility transport is different from a 911 scene response. The sending team usually identifies the patient’s condition, current monitoring needs, and any treatment likely to be needed during the ride.
A stable patient with mobility limits or a straightforward orthopedic issue may be appropriate for BLS. A patient needing continuous cardiac monitoring, airway support, or medication management may require ACLS.
Can a BLS ambulance be upgraded in the field
Yes, in many systems. Crews can request ACLS intercept, rendezvous with a paramedic unit, or upgrade transport based on patient assessment.
That’s a normal part of tiered EMS design. Good BLS crews don’t hesitate to ask for more help when the patient’s condition calls for it.
Is ACLS always faster or better in an emergency
Not automatically. ACLS offers more interventions. Better outcomes depend on whether those interventions are needed and whether they help more than they delay.
That’s the key lesson in the bls vs acls ambulance debate. The best response is the one that fits the patient, the problem, and the clock.
If you need a flexible way to earn or renew certifications, ProMed Certifications offers fully online courses for BLS, ACLS, PALS, CPR, and more. Their platform is built for working healthcare professionals who need credible, convenient training that fits real schedules.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)