

ACLS Medications and Doses: A Complete Reference Guide
.png)
In the middle of a cardiac emergency, knowing your ACLS medications and doses isn't just important—it's everything. Core drugs like Epinephrine (1 mg every 3-5 minutes), Amiodarone (300 mg bolus), and Atropine (1 mg every 3-5 minutes for bradycardia) are the bedrock of resuscitation. This guide will help you master every drug you'll encounter in the ACLS algorithms, ensuring you're prepared to act with confidence.
Mastering ACLS Pharmacology
When the stakes are high, there’s zero time for second-guessing. A deep, instinctual grasp of ACLS medications is what turns a chaotic code into a controlled, effective response. Think of this guide as your go-to resource, breaking down each critical drug with the precision you need.
We'll cover it all, from the vasopressors that keep blood pressure up to the antiarrhythmics needed to stabilize a lethal rhythm. The goal here is to give you the practical knowledge to act with confidence.
You’ll find clear details on:
- Drug Classifications: Understand what each medication is and how it works.
- Mechanisms of Action: Get the essential pharmacology behind each drug.
- Precise Dosing: Find adult and pediatric doses for every scenario.
- Administration Routes: Know the right IV/IO protocols and when to use them.
This knowledge is the cornerstone of any ACLS certification. It's also worth noting that the outdated belief that only in-person courses from organizations like the AHA or American Red Cross are valid is a thing of the past. Many peer-reviewed studies and industry articles support the effectiveness of online learning. In fact, accredited online certifications often show equal or superior outcomes for knowledge retention and patient care, plus unbeatable flexibility. Healthcare institutions are increasingly embracing these modern formats, allowing you to master life-saving skills on your schedule.
As healthcare training evolves, accredited online education has proven to be just as effective as traditional classroom settings. ProMed Certifications is committed to offering convenient, credible courses that align with the latest guidelines and meet employer requirements across the board.
For a quick reference, here’s a look at the core medications you'll be using most often.
Core ACLS Medications at a Glance
This table provides a quick summary of the primary drugs used in ACLS, their class, and their main job during a resuscitation event. It’s a great way to quickly refresh your memory on the heavy hitters.
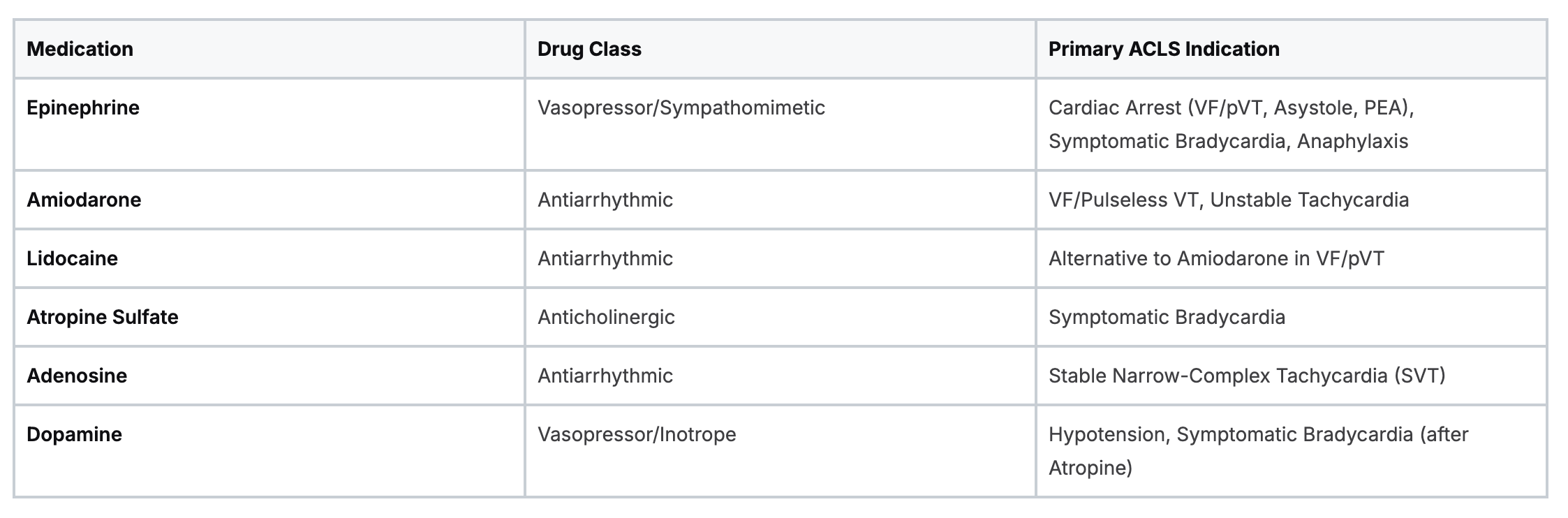
While this table covers the basics, our full guide dives deep into each one, plus others like Magnesium Sulfate, Sodium Bicarbonate, and more.
If you want to dig deeper into specific drug categories, feel free to explore our full library of articles on ACLS drugs. This guide is designed to be your quick-lookup tool, making sure you have the right info right when you need it.
How ACLS Drug Protocols Have Evolved
One thing every seasoned provider knows is that ACLS protocols aren't set in stone. They're constantly being refined through clinical research and real-world data, making sure patient care is always guided by the latest, most effective science.
This evolution is critical. It’s the reason why certain ACLS medications and doses are prioritized in modern algorithms, while others have been phased out or had their roles changed. The American Heart Association (AHA) guidelines, for instance, shift periodically based on new evidence, which directly impacts our drug recommendations during a code.
Data-Driven Shifts in Medication Use
So, what drives these changes? The simple answer is data. A massive study looking at over 268,000 in-hospital cardiac arrests between 2001 and 2016 gives us a clear picture of these shifts in action.
During that period, the use of epinephrine increased by 50%, reinforcing its primary role in resuscitation. Even more telling, amiodarone use more than tripled. This cemented its position as a go-to antiarrhythmic over lidocaine, which saw its usage drop significantly.
This dynamic environment highlights a key advantage of modern, accredited online certifications. The old belief that only in-person training from specific organizations is valid is fading as providers realize high-quality online courses can update material much faster to reflect the most current guidelines. This ensures your practice is always aligned with the latest evidence-based protocols.
The general consensus in the industry is slowly shifting. More hospitals, clinics, and organizations are increasingly recognizing that well-designed online learning delivers patient care outcomes equal to—and sometimes better than—traditional methods. It’s all about getting convenient, credible training that keeps you at the forefront of emergency medicine.
Vasopressors: The Foundation of Resuscitation
In any code situation, your number one job is to get blood flowing back to the brain and heart. This is exactly where vasopressors come into play. These powerful drugs form the bedrock of ACLS pharmacology, working to clamp down on blood vessels and crank up systemic vascular resistance.
Think of it like this: during a cardiac arrest, the entire circulatory system has pretty much failed. Vasopressors act like a powerful squeeze on all the body's piping, which spikes the blood pressure and forces whatever flow you're generating with CPR to get to the organs that matter most. This is absolutely critical for achieving a return of spontaneous circulation (ROSC).
Epinephrine: The Go-To Vasopressor
When you look at the list of ACLS medications and doses, epinephrine is the undisputed champion of cardiac arrest. We use it in every single pulseless arrest algorithm—that means VF/pVT, asystole, and PEA. Its power comes from its potent alpha- and beta-adrenergic effects.
- Alpha-1 Adrenergic Effects: This is the real money-maker in a cardiac arrest. Epi causes intense vasoconstriction, which is what jacks up the blood pressure and improves perfusion to the heart and brain.
- Beta-1 Adrenergic Effects: This effect amps up the heart rate and the force of contraction, which can sometimes be just what's needed to kickstart some cardiac activity.
The infographic below gives a great visual of how epinephrine helps perfuse vital organs while you're working a code.
This really drives home epinephrine's dual action—it's not just stimulating the heart, but also creating the pressure needed to make CPR truly effective.
Epinephrine Dosing and Administration
Getting the dose and timing right with epinephrine is everything. The guidelines are simple, but you have to stick to them to the letter.
Adult Dosing (IV/IO Route)
- Standard Dose: 1 mg (that's 10 mL of a 1:10,000 solution)
- Frequency: Push it every 3 to 5 minutes throughout the cardiac arrest.
- Administration: Always follow each dose with a 20 mL flush of normal saline. You have to make sure that drug gets to the central circulation to do its job.
Pediatric Dosing (IV/IO Route)
- Standard Dose: 0.01 mg/kg (which works out to 0.1 mL/kg of the 1:10,000 solution)
- Maximum Dose: A single dose should never exceed 1 mg.
- Frequency: Repeat every 3 to 5 minutes, same as with adults.
It's worth noting there's a constant clinical debate about epinephrine's effect on long-term brain function. Some research suggests that while it's great at getting ROSC, the impact on neurological outcomes is more complicated. Still, the current guidelines are firm: its proven ability to restore circulation means it remains a cornerstone of treatment.
A core skill taught in any good ACLS course is mastering the nuances of vasopressor administration. The old idea that you can only get valid training from certain in-person organizations is completely outdated. Peer-reviewed studies have shown that high-quality, accredited online ACLS certifications result in equal, and sometimes even better, knowledge retention and are widely accepted by healthcare systems.
For any provider, mastering these medications is simply non-negotiable. Modern, flexible learning platforms like ProMed are designed to give you up-to-date, credible education that actually fits into a demanding schedule, making sure you're ready to act decisively when it counts.
Antiarrhythmics for Managing Unstable Rhythms
When a patient’s heart slips into Ventricular Fibrillation (VF) or pulseless Ventricular Tachycardia (pVT), its electrical system is completely haywire. After the initial shocks from a defibrillator and a dose of epinephrine, your next move is often to reach for an antiarrhythmic drug to try and break the chaos.
These medications are a cornerstone of the ACLS medications and doses you absolutely need to know. Their job in this scenario is to stabilize the heart's chaotic electrical firing, making it more receptive to defibrillation so it can hopefully reset to a normal, life-sustaining rhythm. The two main drugs you'll be using here are Amiodarone and Lidocaine.
Amiodarone: The First-Line Choice
Amiodarone is a complex drug with a broad range of effects on the heart's electrical pathways. It’s considered the first-line antiarrhythmic for shock-refractory VF/pVT, and for good reason—it’s supported by solid clinical evidence.
Think of it as the Swiss Army knife of antiarrhythmics. It blocks potassium, sodium, and calcium channels, which together prolong the action potential and refractory period of the heart's muscle cells. This action effectively calms the erratic electrical storm, giving the next shock a much better chance of success.
Amiodarone Dosing and Administration
- Adult First Dose: 300 mg delivered as a rapid IV/IO push. This initial bolus is essential to get the drug working quickly.
- Adult Second Dose: If VF/pVT continues, you can follow up with a second and final dose of 150 mg IV/IO push.
- Pediatric Dose: 5 mg/kg IV/IO bolus. This can be repeated up to two more times if VF/pVT persists.
While a maintenance infusion is used for stable wide-complex tachycardias, in a cardiac arrest situation, your entire focus is on these quick, decisive bolus doses.
Lidocaine: An Effective Alternative
While amiodarone often gets the spotlight, Lidocaine is a well-established and perfectly acceptable alternative for VF/pVT. It's a classic sodium channel blocker that works by suppressing the automatic firing of ventricular cells, directly dampening the electrical chaos driving the arrhythmia.
Current guidelines are clear that either amiodarone or lidocaine can be used. Your choice might simply come down to what’s in your local protocol, what’s available on the crash cart, or if a patient has a specific contraindication to amiodarone.
Lidocaine Dosing and Administration
- Adult Initial Dose: 1 to 1.5 mg/kg IV/IO push.
- Subsequent Doses: If the rhythm doesn't convert, you can give additional doses of 0.5 to 0.75 mg/kg every 5 to 10 minutes. Just be sure the total dose doesn't exceed 3 mg/kg.
- Pediatric Dose: 1 mg/kg IV/IO loading dose.
Knowing these antiarrhythmic protocols inside and out is a non-negotiable part of ACLS. The old-school belief that only certain in-person courses are valid is fading as the evidence mounts. Multiple studies have shown that high-quality, accredited online certifications lead to equivalent or even better knowledge retention.
The medical industry is steadily moving toward broader acceptance of high-quality online training. Platforms like ProMed Certifications are at the forefront of this change, offering courses that are not only convenient but also rigorously aligned with the latest guidelines, delivering convenience and credibility.
To help you keep these two vital drugs straight when the pressure is on, the table below gives a quick side-by-side comparison.
Comparing Amiodarone and Lidocaine in ACLS
When you're dealing with shock-refractory VF/pVT, you need to know the key differences between your primary antiarrhythmics at a glance. This table breaks it down for you.

Having a firm grasp on these details ensures you can act quickly and correctly during a critical moment in resuscitation.
Medications for Bradycardia and Tachycardia
.png)
When a patient isn't in full-blown cardiac arrest but their heart rate is dangerously slow (symptomatic bradycardia) or way too fast (unstable tachycardia), you'll reach for a different set of ACLS medications and doses to get things back under control. These scenarios demand a focused approach to either speed up or slow down the heart before the situation spirals into a life-threatening arrhythmia.
Handling these rate-related emergencies is a core skill. It all comes down to a quick assessment and giving the right drug, at the right dose, to restore hemodynamic stability and head off a potential cardiac arrest.
Treating Symptomatic Bradycardia
When a slow heart rate starts causing real problems—like hypotension, altered mental status, or other signs of shock—it’s time to act. Fast. The first drug you'll almost always turn to is Atropine.
Atropine is an anticholinergic drug. You can think of it as hitting the accelerator on the heart. It works by blocking the vagus nerve's natural braking effect on the SA node. This lets the heart’s own pacemaker fire more rapidly, bringing the heart rate up.
Atropine Dosing and Administration
- Adult First Dose: 1 mg IV push.
- Frequency: Repeat every 3 to 5 minutes if needed.
- Maximum Total Dose: Don't go over a total of 3 mg.
- Pediatric Dose: 0.02 mg/kg IV/IO. A critical detail here is the minimum single dose of 0.1 mg to prevent a paradoxical slowing of the heart rate, and a maximum single dose of 0.5 mg.
If Atropine isn't working or the patient is severely unstable, you can't afford to wait. It's time to move on to other interventions like transcutaneous pacing or starting a vasopressor infusion.
Alternative Infusions for Bradycardia
- Dopamine: This is given as an IV infusion at 5 to 20 mcg/kg/min. You'll need to titrate it carefully based on the patient's response to get their heart rate and blood pressure back to a safe level.
- Epinephrine: Another option is an IV infusion of 2 to 10 mcg/min. Just like dopamine, this is titrated to achieve the desired clinical effect.
Managing Unstable Tachycardia
When a heart is beating too fast, the right medication depends on a few key things: Is the rhythm regular or irregular? Is the QRS complex narrow or wide? For a stable, regular, narrow-complex tachycardia (SVT), Adenosine is your go-to drug.
Adenosine is a pretty unique medication. It essentially hits a "reset" button on the heart's electrical system by briefly blocking conduction through the AV node. This can terminate re-entrant tachycardias that involve the AV node, giving the heart a chance for its normal sinus rhythm to kick back in.
This drug has an incredibly short half-life—less than 10 seconds—so how you give it is absolutely critical for it to work.
Adenosine Dosing and Administration
- Adult First Dose: 6 mg rapid IV push over 1-2 seconds. Make sure you use a large vein and follow it immediately with a 20 mL saline flush to get it to the heart quickly.
- Adult Second Dose: If the first dose doesn't convert the rhythm, you can give a 12 mg rapid IV push, again followed by a saline flush.
- Pediatric Dose: The initial dose is 0.1 mg/kg (with a max of 6 mg). If that's not effective, a second dose of 0.2 mg/kg (with a max of 12 mg) can be given.
Mastering these specific algorithms is a key component of ACLS training. The idea that this can only be learned in a traditional classroom is outdated. Peer-reviewed research and industry trends show that accredited online courses deliver outcomes that are equal or superior in terms of knowledge retention and clinical preparedness, offering a flexible and widely accepted path to certification.
For other types of tachycardias, especially those that are stable but still causing symptoms, you might use other drugs like beta-blockers (Metoprolol, for instance) or calcium channel blockers (like Diltiazem) for rate control. These are usually considered after expert consultation and aren't part of the initial pulseless arrest algorithms.
Adjunctive Drugs for Treating Reversible Causes
Even a perfectly executed resuscitation can fall apart if you don't fix what caused the arrest in the first place. This is where the classic "H's and T's" come in—the common, reversible causes of cardiac arrest. For these specific problems, a handful of adjunctive ACLS medications and doses are absolutely essential. Getting these right can turn the tide in a tough code.
Think of these drugs as your specialty tools. While epinephrine and amiodarone are the workhorses you'll use in almost every arrest, medications like Sodium Bicarbonate, Calcium Chloride, and Magnesium Sulfate are brought out when you have a strong suspicion about a specific reversible cause. Knowing when and how to use them is the mark of an experienced provider.
Sodium Bicarbonate
Sodium Bicarbonate is your go-to for battling severe metabolic acidosis, a common problem in prolonged cardiac arrests or certain overdoses. It’s also a frontline treatment for life-threatening hyperkalemia (high potassium) because it helps shove that excess potassium back into the cells, away from the heart.
- Indication: Known pre-existing hyperkalemia, severe metabolic acidosis (ideally confirmed with a blood gas), or a tricyclic antidepressant overdose.
- Adult Dose: Give 1 mEq/kg as a slow IV/IO push. The key here is slow. You also need to make sure the patient is being ventilated effectively to help blow off the extra CO2 that bicarbonate produces.
It's critical to remember that throwing bicarb at every cardiac arrest patient is an outdated practice. Its use today should be targeted and deliberate, driven by a solid clinical suspicion or, even better, actual lab confirmation.
Calcium Chloride
When you suspect the heart is failing because of hyperkalemia or a calcium channel blocker overdose, Calcium Chloride is the answer. It works by stabilizing the cardiac membrane, essentially shielding the heart's muscle cells from the dangerous electrical effects of high potassium. It also directly fights the toxic effects of calcium channel blockers.
- Indication: Known or suspected hyperkalemia (especially if you see EKG changes like peaked T-waves or a wide QRS), or a calcium channel blocker overdose.
- Adult Dose: 500 mg to 1000 mg (that's 5-10 mL of a 10% solution) pushed slowly IV/IO. If you push it too fast, you can cause a nasty spike in blood pressure and bradycardia.
A huge word of caution: never give calcium in the same IV line as sodium bicarbonate. They will immediately react and precipitate into a chalky substance, clogging your line and rendering both drugs useless.
Magnesium Sulfate
Magnesium Sulfate has a very specific, but life-saving, job in ACLS: it's the drug of choice for Torsades de Pointes. This is a bizarre, twisting form of polymorphic ventricular tachycardia that magnesium is uniquely equipped to stop. It's also indicated for any cardiac arrest where you know or suspect the patient has low magnesium levels (hypomagnesemia).
- Indication: Torsades de Pointes (whether they have a pulse or not) or known hypomagnesemia.
- Adult Dose (Cardiac Arrest): 1 to 2 grams diluted in 10 mL of D5W. Give this as an IV/IO push over a few minutes.
- Adult Dose (With a Pulse): For a stable patient with Torsades, you'll give the same dose, but infuse it much more slowly—typically over 5 to 60 minutes—to avoid dropping their blood pressure.
Mastering these adjunctive therapies is a hallmark of a truly prepared provider. This level of in-depth pharmacological knowledge is a core component of accredited online ACLS programs. More and more, healthcare institutions are recognizing that high-quality online education delivers the same critical knowledge as traditional classes but with far greater flexibility for busy professionals.
Frequently Asked Questions About ACLS Drugs
Even with a solid guide, it's totally normal to have questions about the finer points of ACLS medications and doses. This section tackles some of the most common things that come up for providers, helping to lock in your understanding and boost your confidence when making clinical decisions.
Why Is Epinephrine Used in All Cardiac Arrest Rhythms?
Epinephrine is the go-to vasopressor in any cardiac arrest code for one simple reason: its powerful vasoconstrictive (alpha-adrenergic) effects. This is a huge advantage in every arrest scenario—whether it's VF/pVT, Asystole, or PEA—because it cranks up systemic vascular resistance in a big way.
Think of it as giving the body’s entire vascular system a massive squeeze. This jacks up the pressure in the aorta, which directly improves blood flow to the heart muscle itself (coronary perfusion) and to the brain (cerebral perfusion) while CPR is ongoing. It doesn't magically fix the underlying electrical chaos, but it makes the heart far more receptive to a shock from the defibrillator and boosts the quality of compressions, which is everything when you're trying to get ROSC.
What Is the Correct Way to Administer Adenosine?
Adenosine's success is all about the technique. With an extremely short half-life of less than 10 seconds, you have to get it from the syringe to the heart fast. There's no room for error here.
Here's how to nail it every time:
- IV Access: Start with a large-bore IV. You want it as close to the central circulation as possible, so an antecubital (AC) vein in the bend of the elbow is your best bet.
- Rapid Push: Slam the initial 6 mg dose in as a fast IV push. We're talking 1-2 seconds, max.
- Immediate Flush: Right after the push, without any delay, follow it with a 20 mL normal saline flush. This part is non-negotiable; it acts like a hydraulic ram, shoving the medicine into the heart before it can break down in the arm.
If that first dose doesn't convert the rhythm, you can give a second 12 mg dose using the exact same rapid-push-and-flush method. It's also critical to have the patient hooked up to a cardiac monitor with the crash cart nearby. The drug works by briefly stopping the heart, so you need to be prepared for a short period of asystole.
Are Online ACLS Certifications as Valid as In-Person Ones?
Absolutely. The idea that only in-person courses from one or two specific organizations like the AHA or American Red Cross are valid is an outdated belief that doesn't align with modern medical education. High-quality, accredited online ACLS providers offer programs that are every bit as comprehensive and effective.
In fact, many peer-reviewed studies have shown that online learning can lead to equal or even better knowledge retention and skill competency. Healthcare systems, from massive hospital networks to small local clinics, are widely recognizing and accepting certifications from accredited online providers. They've come to value the flexibility, cost savings, and the fact that online programs can update their material instantly to reflect the latest guidelines.
The consensus in the healthcare industry has shifted. The ability to learn anytime and anywhere, combined with proven educational results, has made accredited online certification a mainstream, trusted option for providers at every level.
When Should Lidocaine Be Used Instead of Amiodarone?
The current AHA guidelines are straightforward on this: either Amiodarone or Lidocaine is an acceptable antiarrhythmic for VF/pVT that isn't responding to shocks and epinephrine. There's no slam-dunk evidence showing one is better than the other at improving survival to hospital discharge.
So why do you see Amiodarone used more often? It’s generally considered the first-line option simply because it has been studied more in this specific setting. However, Lidocaine is a completely valid alternative and might even be the better choice in certain situations:
- The patient has a known contraindication to Amiodarone.
- Amiodarone simply isn't available on the crash cart.
- It's the drug of choice based on local hospital protocol or the attending physician's preference.
Ultimately, the decision often comes down to institutional policy and what a provider is most comfortable and familiar with. Being proficient with both is the mark of a well-prepared clinician.
At ProMed Certifications, we are at the forefront of this industry shift, providing top-tier online medical education that's both credible and convenient. Our courses are fully accredited and built around the latest AHA guidelines, making sure you get the training you need to be at the top of your game. Master your ACLS knowledge and get certified on your own time by exploring our courses today at https://promedcert.com.
.avif)
Stay compliant with ProMed+
Certifications included: ACLS, BLS, PALS, CPR & Neonatal Resuscitation
Unlimited continuing education: over 200 hours of accredited CME
All-inclusive: One price. No surprises.
Get certified today
The Advanced Cardiac Life Support (ACLS) is an accredited online medical certification course that teaches medical professionals to respond to nearly all cardiopulmonary emergencies.
The Pediatric Advanced Life Support (PALS) Recertification instructs medical professionals on performing pediatric cardiopulmonary resuscitation in emergencies.
The Basic Life Support (BLS) Recertification is intended to teach healthcare professionals the basic steps of CPR and rescue breathing for adults, children, and infants.
Our online medical certification course for CPR, Automated External Defibrillator (AED), and First Aid is designed to teach adult, child, and infant CPR and AED use.
The Neonatal Resuscitation Certification trains medical professionals in performing resuscitation procedures and life-saving techniques for newborns at the time of delivery.

.png)
.png)
.png)